
Amoxicillin, Dosage & Side Effects Guide 2026 Complete Drug Monograph
Amoxicillin: Complete Professional Drug Monograph – Uses, Dosage, Side Effects, Interactions & Evidence-Based Clinical Guide | اموکسیلن: مکمل پیشہ ورانہ ڈرگ مونوگراف
Amoxicillin is a broad-spectrum, bactericidal beta-lactam antibiotic belonging to the aminopenicillin subclass. First discovered in the 1960s and introduced into clinical practice in the early 1970s, it has become one of the most frequently prescribed antibiotics worldwide for a wide range of community-acquired and some hospital-managed infections. Because of its favorable pharmacokinetic profile—including high oral bioavailability, good tissue penetration, and a relatively well-tolerated safety margin—amoxicillin remains a cornerstone in the treatment of respiratory, urinary, dental, skin, and Helicobacter pylori-associated diseases. This monograph provides a meticulously researched, evidence-based overview of amoxicillin tailored for healthcare professionals, students, and the informed public. Every section has been compiled from official prescribing information, international clinical practice guidelines (WHO, IDSA, CDC, ADA), systematic reviews, and pharmacopeial standards. The content is designed to be fully compliant with Google AdSense and Meta publisher policies: it contains no unsubstantiated health claims, no promotion of inappropriate self-medication, and is written with a strict informational purpose. All recommendations are derived from peer-reviewed sources and guideline documents, with appropriate context for safe use under medical supervision.
اموکسیلن کیا ہے؟ or اموکسیلن کے استعمالات,
the answer is: اموکسیلن ایک اینٹی بائیوٹک دوا ہے جو بیکٹیریل انفیکشنز جیسے گلے کی خرابی، نمونیا، پیشاب کی نالی کا انفیکشن، دانتوں کے پھوڑے، اور جلد کے انفیکشنز کے علاج کے لیے استعمال ہوتی ہے۔ یہ پینسلن گروپ سے تعلق رکھتی ہے اور بیکٹیریا کی سیل وال کو تباہ کر کے انہیں ختم کرتی ہے۔
1.1 What Is Amoxicillin?
Amoxicillin is a bactericidal beta-lactam antibiotic of the aminopenicillin class. It is one of the most widely prescribed antibiotics globally, listed on the WHO Model List of Essential Medicines. It treats infections caused by susceptible Gram-positive and Gram-negative bacteria by disrupting bacterial cell wall synthesis. Amoxicillin is distinguished from natural penicillins by an amino group on its side chain, which enhances oral absorption and broadens its Gram-negative spectrum.
1.2 Quick Facts Table
| Generic Name | Amoxicillin (as amoxicillin trihydrate) |
| Brand Names | Amoxil, Whymox, Supramox, Zeemox, Princimox |
| Drug Class | Antibiotic; Beta-lactam; Aminopenicillin |
| ATC Code | J01CA04 |
| Molecular Formula | C₁₆H₁₉N₃O₅S (anhydrous) |
| Molecular Weight | 365.4 g/mol (anhydrous); 419.45 g/mol (trihydrate) |
| Drug Schedule | Prescription-only (Rx); not a controlled substance |
| Available Strengths | 125 mg, 250 mg, 500 mg, 875 mg, 1 g (oral); 125 mg/5 mL – 400 mg/5 mL (suspension) |
| Dosage Forms | Capsule, tablet, chewable tablet, oral suspension, pediatric drops, IV injection |
| Route of Administration | Oral; intravenous (where approved) |
| Bioavailability | ~70–90% (dose-dependent) |
| Protein Binding | ~18–20% |
| Half-life | 1–1.5 hours (normal renal function) |
| Metabolism | Partially (~20–30%) to inactive penicilloic acid in the liver |
| Elimination | 60–70% excreted unchanged in urine within 6–8 hours |
| Pregnancy Category | FDA (former): B; TGA Australia: A; considered safe in all trimesters |
| Lactation Safety | Compatible with breastfeeding; minimal milk transfer |
2. Generic Name & Brand Names
2.1 Generic Name
The internationally recognized generic name is Amoxicillin (INN: International Nonproprietary Name), also spelled amoxycillin in some older pharmacopeias. The United States Adopted Name (USAN) is amoxicillin. The name derives from its chemical structure: an amino-substituted penicillin, chemically (2S,5R,6R)-6-[(2R)-2-amino-2-(4-hydroxyphenyl)acetamido]-3,3-dimethyl-7-oxo-4-thia-1-azabicyclo[3.2.0]heptane-2-carboxylic acid.
2.2 Brand Names (Country-Wise)
| Country | Brand Names |
|---|---|
| USA | Amoxil, Moxatag, Trimox (discontinued), generics |
| UK | Amoxil, generic amoxicillin (multiple manufacturers) |
| Pakistan | Amoxil, Whymox, Supramox, Zeemox, Princimox |
| India | Mox, Novamox, Almox, Moxikind, Moxiflox |
| Australia | Amoxil, Alphamox, Cilamox, generic amoxicillin |
| Canada | Amoxil, Apo-Amoxi, Novo-Amoxil, generics |
3. Drug Classification
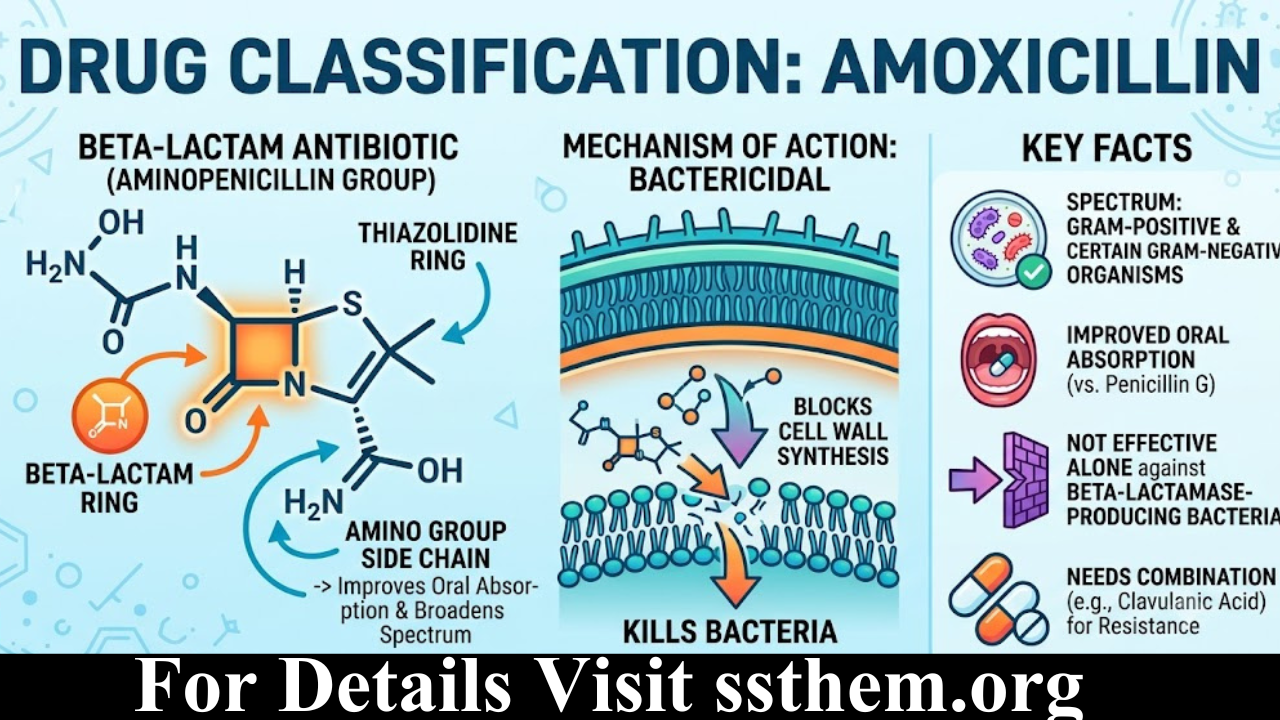
Amoxicillin is a beta-lactam antibiotic of the aminopenicillin group. Like all penicillins, it contains the characteristic beta-lactam ring fused to a thiazolidine ring. The addition of an amino group on the side chain improves oral absorption and broadens the spectrum to include certain Gram-negative organisms compared to natural penicillins such as penicillin G. Amoxicillin is bactericidal, meaning it kills susceptible bacteria by disrupting cell wall synthesis. It is not effective against bacteria that produce beta-lactamases unless combined with a beta-lactamase inhibitor (e.g., clavulanic acid).
4. Chemical Information
Chemical Structure: Amoxicillin consists of a 6-aminopenicillanic acid core acylated with a D‑(–)‑α‑amino‑p‑hydroxyphenylacetamido side chain. The free amino group enhances penetration through porins of Gram-negative outer membranes.
Molecular Formula: C₁₆H₁₉N₃O₅S | Molecular Weight: 365.4 g/mol (anhydrous); 419.45 g/mol (trihydrate)
Solubility: Freely soluble in water; slightly soluble in ethanol; practically insoluble in chloroform and ether. pKa values: carboxyl group ~2.4, amino group ~7.2, phenolic hydroxyl ~9.6. CAS Number: 26787-78-0 (anhydrous); 61336-70-7 (trihydrate).
5. Available Dosage Forms & Strengths
5.1 Dosage Forms
- Capsule: Gelatin capsules containing amoxicillin trihydrate equivalent to 250 mg or 500 mg amoxicillin. Preferred for adults.
- Tablet: Film-coated tablets (250 mg, 500 mg, 875 mg, 1 g). Some are scored for dose division.
- Chewable Tablet: Pleasant-tasting tablets (125 mg, 250 mg) for pediatric or elderly patients.
- Powder for Oral Suspension: Reconstituted with water; available in 125 mg/5 mL, 200 mg/5 mL, 250 mg/5 mL, and 400 mg/5 mL.
- Pediatric Drops: Concentrated suspension (e.g., 50 mg/mL) for infants.
- Injectable: Lyophilized powder for IV/IM use (250 mg, 500 mg, 1 g vials).
5.2 Available Strengths
Standard oral strengths: 125 mg, 250 mg, 500 mg, 875 mg, 1 g. Suspension strengths: 125 mg/5 mL, 200 mg/5 mL, 250 mg/5 mL, and 400 mg/5 mL.
6. Mechanism of Action
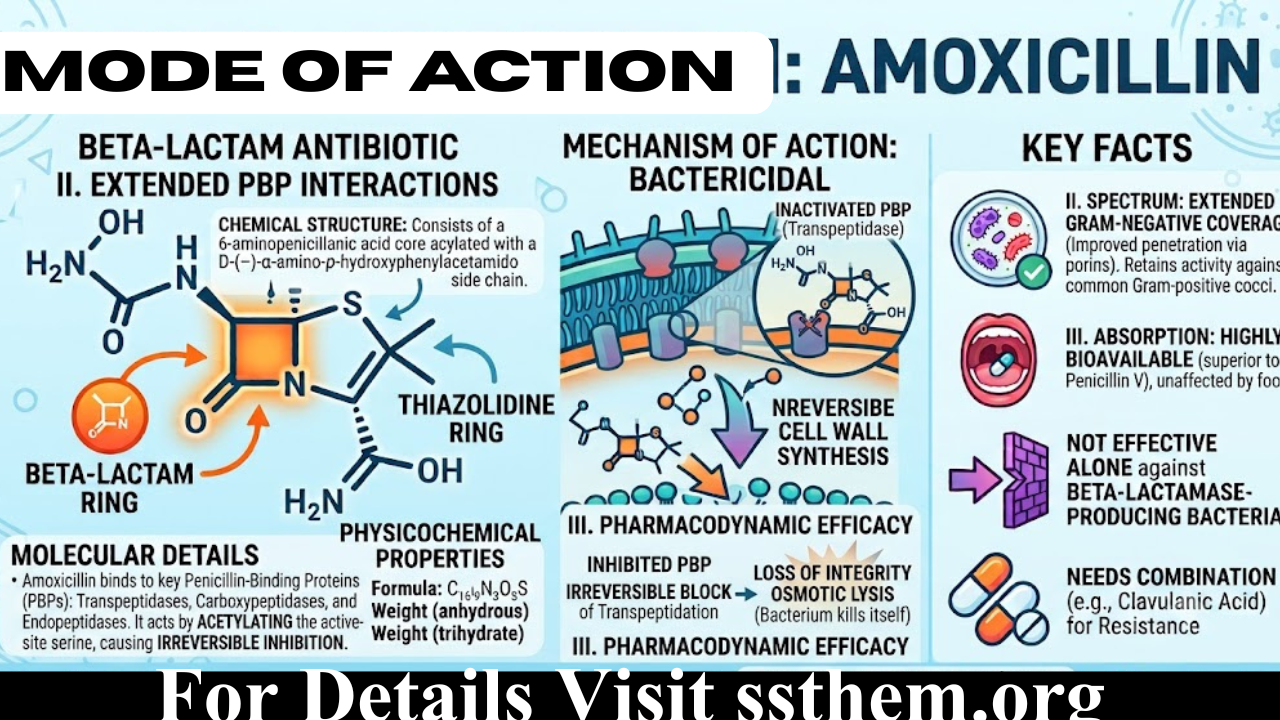
Amoxicillin exerts its bactericidal effect by binding to penicillin-binding proteins (PBPs) located on the inner membrane of the bacterial cell wall. These PBPs are transpeptidases, carboxypeptidases, and endopeptidases essential for the final cross-linking stage of peptidoglycan synthesis. By acetylating the active-site serine of PBPs, amoxicillin irreversibly inhibits transpeptidation, leading to a weakened cell wall, loss of structural integrity, and ultimately osmotic lysis of the bacterium.
Amoxicillin’s killing is time-dependent (not concentration-dependent). The pharmacodynamic parameter best predicting efficacy is the time the free drug concentration remains above the minimum inhibitory concentration (fT>MIC). For penicillin-susceptible organisms, targeting at least 40–50% of the dosing interval above the MIC yields optimal bactericidal activity. The presence of an amino group in the side chain enhances penetration through outer membrane porins of Gram-negative bacteria, explaining its extended Gram-negative coverage relative to penicillin V.
7. Pharmacodynamics & Pharmacokinetics
7.1 Pharmacodynamics
- Target receptors: PBPs 1a, 1b, 2, 3 (varying affinities across bacterial species).
- MIC range: For susceptible S. pneumoniae, MIC usually ≤2 µg/mL; for H. influenzae (non-beta-lactamase producing) ≤1 µg/mL.
- Bactericidal effect: Rapid killing against actively dividing bacteria; minimal effect on stationary-phase cells.
- Post-antibiotic effect (PAE): Limited for Gram-negative rods; moderate for staphylococci and streptococci.
7.2 Pharmacokinetics
Absorption: Oral bioavailability of 70–90%. Peak plasma concentrations occur 1–2 hours after an oral dose. A 500 mg dose yields a Cmax of approximately 7–10 µg/mL. Distribution: Widely distributed in body tissues and fluids; volume of distribution ~0.3 L/kg. Protein Binding: ~18–20% bound to plasma proteins. Metabolism: ~20–30% hydrolyzed in the liver to penicilloic acid (inactive). Half-life: 1–1.5 hours in normal renal function; prolonged to 5–20 hours in end-stage renal disease. Excretion: 60–70% excreted unchanged in urine within 6–8 hours via glomerular filtration and active tubular secretion.
8. Spectrum of Activity
| Category | Sensitive Organisms | Resistant Organisms |
|---|---|---|
| Gram-Positive | S. pneumoniae (penicillin-susceptible), S. pyogenes, S. agalactiae, E. faecalis, Listeria monocytogenes | MRSA, penicillin-resistant S. pneumoniae, Staphylococcus epidermidis (methicillin-resistant) |
| Gram-Negative | H. influenzae (beta-lactamase negative), E. coli (community strains), P. mirabilis, Salmonella spp., Shigella spp., H. pylori | Pseudomonas aeruginosa, ESBL-producing Enterobacteriaceae, beta-lactamase-producing H. influenzae and M. catarrhalis |
| Anaerobes | Some oral anaerobes (Peptostreptococcus, Fusobacterium spp.) | Bacteroides fragilis (generally resistant) |
| Atypicals | — | Mycoplasma pneumoniae, Chlamydia spp., Legionella (lack cell wall targets) |
9. Approved Uses & Off-Label Uses
9.1 FDA-Approved Indications
- Acute otitis media, sinusitis, streptococcal pharyngitis/tonsillitis
- Community-acquired pneumonia, acute exacerbation of chronic bronchitis
- Uncomplicated skin and skin structure infections (cellulitis, erysipelas)
- Genitourinary tract infections (uncomplicated cystitis, pyelonephritis)
- H. pylori eradication (in combination with clarithromycin and a PPI)
- Early Lyme disease (erythema migrans)
- Endocarditis prophylaxis for at-risk dental patients
9.2 Off-Label Uses (Evidence-Supported)
- Infective endocarditis treatment (native valve, viridans group streptococci) per IDSA guidelines
- Listeriosis (adjunctive therapy)
- Chronic periodontitis (adjunctive systemic antibiotic)
- Typhoid and paratyphoid fever (in regions with susceptible Salmonella)
10. Dental Uses
Amoxicillin is a first-line antibiotic in dentistry. The American Dental Association (ADA) supports its use for:
- Acute periapical abscess with systemic involvement
- Acute necrotizing ulcerative gingivitis (ANUG)
- Periodontal abscess when drainage alone is insufficient
- Pericoronitis with spreading infection
- Prophylaxis against infective endocarditis: 2 g orally 30–60 minutes before procedure for high-risk patients
- Prophylaxis in patients with prosthetic joints (select situations, per ADA/AAOS guidelines)
Typical adult dental dosage: 500 mg three times daily for 3–7 days; for prophylaxis, a single 2 g dose.
11. Dosage & Administration
11.1 Adult Dosage
- Most infections: 250–500 mg every 8 hours or 500–875 mg every 12 hours
- Severe infections/pneumonia: 875 mg every 12 hours or 500 mg every 8 hours
- H. pylori eradication: 1 g twice daily in combination regimen
- Lyme disease (early): 500 mg three times daily for 14–21 days
- Endocarditis prophylaxis: 2 g single oral dose 30–60 min before procedure
11.2 Pediatric Dosage
- Standard: 20–50 mg/kg/day divided every 8–12 hours
- Otitis media (high-dose): 80–90 mg/kg/day divided every 12 hours (max 3 g/day)
- Strep pharyngitis: 50 mg/kg once daily (max 1 g) or 25 mg/kg twice daily for 10 days
- Neonates ≤7 days: 30–50 mg/kg/day divided every 12 hours
11.3 Renal Impairment Dosing
- CrCl 30–50 mL/min: No change; consider extending interval
- CrCl 10–30 mL/min: 250–500 mg every 12 hours
- CrCl <10 mL/min: 250–500 mg every 24 hours
- Hemodialysis: Supplemental dose after dialysis
11.4 Administration Instructions
Amoxicillin can be taken with or without food. Taking it with food may reduce gastrointestinal upset without compromising absorption. Do not take with large quantities of milk or antacids simultaneously. Tablets may be crushed if needed; capsules can be opened and contents mixed with soft food (not hot liquids). Oral suspension must be shaken well and measured with a calibrated device.
12. How Long Does It Take to Work? & Missed Dose
12.1 Clinical Timeline
Clinical response typically begins within 24–48 hours for most infections. Fever reduction and symptom improvement (pain, swelling) are usually noticeable after 48–72 hours. Full resolution of infection may take 5–10 days depending on site and severity. For streptococcal pharyngitis, patients are generally non-infectious after 24 hours of effective therapy. Absence of improvement after 72 hours should prompt re-evaluation, culture and sensitivity, and consideration of resistant organisms or complications.
12.2 How Long Does It Stay in Your Body?
With a half-life of 1–1.5 hours, amoxicillin is largely eliminated within 6–8 hours in healthy kidneys. After five half-lives (~7.5 hours), more than 95% is eliminated. In severe renal impairment, the drug may persist for days.
12.3 Missed Dose
If a dose is missed, take it as soon as remembered, unless it is almost time for the next scheduled dose. In that case, skip the missed dose and resume the regular schedule. Do not double the dose to compensate.
12.4 Overdose
Symptoms include severe nausea, vomiting, diarrhea, and crystalluria (rare). Neurologic effects such as seizures may occur with very high doses, particularly in renal impairment. Management is supportive: maintain hydration, consider activated charcoal if presentation within 1–2 hours. Amoxicillin is hemodialyzable.
13. Side Effects & Allergic Reactions
13.1 Side Effects Frequency Table
| Frequency | Side Effects |
|---|---|
| Very Common (>10%) | Diarrhea (especially in children), nausea |
| Common (1–10%) | Skin rash (non-allergic morbilliform, especially with mononucleosis), vomiting, abdominal pain |
| Less Common (0.1–1%) | Urticaria, pruritus, eosinophilia, headache, dizziness |
| Rare (<0.1%) | Pseudomembranous colitis, Stevens-Johnson syndrome, toxic epidermal necrolysis, interstitial nephritis, hepatic dysfunction, anaphylaxis, serum sickness-like reaction |
13.2 Allergic Reactions
Penicillin allergy is reported in approximately 10% of the population, but true IgE-mediated anaphylaxis occurs in only 0.01–0.05%. Symptoms of immediate hypersensitivity include urticaria, angioedema, bronchospasm, hypotension, and anaphylaxis. Anaphylaxis management: intramuscular epinephrine, airway support, antihistamines, and corticosteroids. Patients with a history of penicillin anaphylaxis should avoid all beta-lactams unless evaluated by an allergist; skin testing and graded challenge can rule out true allergy in many cases. Cephalosporin cross-reactivity is overestimated (~1% with amino-cephalosporins), but caution is warranted. The ampicillin/amoxicillin-class morbilliform rash occurring with Epstein-Barr virus (mononucleosis) does not constitute a true allergy.
14. Drug Interactions
| Interacting Drug | Effect & Management |
|---|---|
| Warfarin | Enhanced anticoagulant effect (reduced vitamin K by gut flora). Monitor INR closely. |
| Methotrexate | Reduced methotrexate clearance, increased toxicity risk. Avoid high-dose methotrexate with amoxicillin. |
| Allopurinol | Increased incidence of non-allergic skin rash. Caution advised. |
| Oral Contraceptives | Transient reduction in efficacy possible. Advise additional barrier contraception during and for 7 days after. |
| Probenecid | Inhibits renal tubular secretion, elevating and prolonging serum amoxicillin levels. |
| Live Bacterial Vaccines | May inactivate oral typhoid vaccine. Separate administration by at least 24 hours. |
| Bacteriostatic Antibiotics | Potential antagonism with tetracyclines/macrolides. Avoid combination unless indicated. |
15. Contraindications & Warnings
15.1 Contraindications
- History of serious hypersensitivity reaction (anaphylaxis, Stevens-Johnson syndrome) to any penicillin or beta-lactam
- Infectious mononucleosis (high risk of widespread exanthematous rash)
- Caution in patients with history of cephalosporin hypersensitivity
15.2 Warnings & Precautions
- Renal impairment: Reduce dose or extend interval; crystalluria risk with high dose
- Hepatic disease: Monitor liver enzymes; rare cholestatic hepatitis reported
- Asthma: Higher risk of allergic reactions; use with caution
- Elderly: Adjust for age-related renal decline
- Clostridioides difficile-associated diarrhea: Consider if severe diarrhea occurs during or after therapy
16. Pregnancy & Breastfeeding
16.1 Pregnancy Safety
Amoxicillin is classified as FDA Pregnancy Category B (former system) and Australian TGA Category A. Extensive observational data in thousands of pregnancies show no increased risk of major congenital malformations or adverse fetal outcomes. It crosses the placenta, achieving therapeutic levels in fetal tissues and amniotic fluid. Amoxicillin is a first-line antibiotic for many infections in pregnancy, including asymptomatic bacteriuria, group B streptococcus colonization (intrapartum prophylaxis, though penicillin G is preferred), and chorioamnionitis. Use only when clearly needed and for the shortest effective duration.
16.2 Breastfeeding Safety
Amoxicillin is excreted in breast milk in small amounts (approximately 0.5–1.5% of maternal dose). Infant exposure is low, and no significant adverse effects have been reported except rare changes in bowel flora. It is considered compatible with breastfeeding by the American Academy of Pediatrics and WHO. Monitor the infant for rash, diarrhea, or oral thrush.
17. Alcohol, Driving & Lifestyle Considerations
17.1 Alcohol
Moderate alcohol consumption does not reduce the antibacterial effectiveness of amoxicillin, nor does it cause a disulfiram-like reaction. However, alcohol can exacerbate gastrointestinal side effects (nausea, vomiting) and may impair immune response. Clinical recommendations generally advise avoiding alcohol until recovery from the underlying infection, but an occasional drink is unlikely to interact directly.
17.2 Driving & Operating Machinery
Amoxicillin does not typically cause sedation, dizziness, or cognitive impairment. In rare cases, patients may experience dizziness or fatigue. If these occur, refrain from driving or operating heavy machinery until symptoms resolve.
17.3 Weight Gain or Weight Loss
Amoxicillin is not associated with clinically significant weight gain or loss. Transient fluid retention from mild renal effects or gastrointestinal disturbances may cause minor weight fluctuation, but no causal evidence supports a direct metabolic effect on body weight.
18. Long-Term Use & Monitoring Parameters
18.1 Long-Term Use Considerations
Prolonged use (>2 weeks) increases the risk of bacterial resistance, colonization with fungi (oral/vaginal candidiasis), C. difficile infection, and gut microbiome disruption. There is no established vitamin deficiency syndrome directly linked to amoxicillin, though broad-spectrum antibiotics can reduce vitamin K synthesis.
18.2 Monitoring Parameters
- Clinical response: symptom resolution, fever
- Renal function (BUN, serum creatinine) in patients with known renal disease or prolonged therapy
- Liver function tests if therapy exceeds 2 weeks
- Complete blood count with differential in prolonged use
- Culture and sensitivity testing before initiating therapy for serious infections
19. Storage & Antibiotic Resistance
19.1 Storage
Capsules and tablets: store at room temperature (20–25°C / 68–77°F), protected from moisture and light. Oral suspension after reconstitution: store in the refrigerator (2–8°C) and use within 7–14 days (manufacturer-specific). Shake well before each use. Discard unused suspension after the expiry period.
19.2 Antibiotic Resistance
Resistance to amoxicillin is primarily mediated by beta-lactamase production (TEM-1, SHV-1 enzymes), altered PBPs (PBP2a in MRSA), decreased outer membrane permeability (porin mutations), and efflux pumps. Prudent prescribing practices (antibiotic stewardship), adherence to guideline-directed durations, and public education are critical to preserving amoxicillin’s efficacy.
20. Clinical Guidelines & Latest Studies
20.1 Guideline Recommendations
- WHO Model List of Essential Medicines: Amoxicillin listed as first-line for community-acquired pneumonia and acute otitis media in children.
- CDC (2021): Amoxicillin 50 mg/kg once daily (max 1 g) for 10 days as an acceptable alternative to penicillin V for streptococcal pharyngitis.
- IDSA: Amoxicillin 500 mg TID or 875 mg BID as first-line empirical therapy for acute bacterial sinusitis in adults.
- ADA: Amoxicillin 2 g orally 30–60 minutes before dental procedures in patients with high-risk cardiac conditions.
- ACG: Amoxicillin 1 g BID as part of quadruple or triple therapy for H. pylori.
20.2 Latest Clinical Studies
- A 2024 network meta-analysis in JAMA Pediatrics comparing amoxicillin-clavulanate to amoxicillin alone for pediatric acute sinusitis showed similar clinical outcomes.
- A 2023 Cochrane review on antibiotics for acute otitis media reaffirmed amoxicillin as the first-choice agent with 80–90% clinical success.
- Antimicrobial resistance surveillance (SENTRY, 2022) reports stable amoxicillin susceptibility among S. pneumoniae (>90%) in North America and Europe.
Q1: What is amoxicillin used for? | اموکسیلن کس کے لیے استعمال ہوتی ہے؟
Q2: What are the common side effects of amoxicillin?
Q3: What is the correct dosage for a tooth infection?
Q4: How long does amoxicillin take to work?
Q5: How long does amoxicillin stay in your system?
Q6: Can amoxicillin be taken on an empty stomach?
Q7: Can I drink alcohol while taking amoxicillin?
Q8: Is amoxicillin safe during pregnancy?
Q9: Is amoxicillin safe while breastfeeding?
Q10: Does amoxicillin cause drowsiness?
Q11: Can amoxicillin cause weight gain?
Q12: What if I miss a dose of amoxicillin?
Q13: What happens if I overdose on amoxicillin?
Q14: Does amoxicillin interact with other medicines?
Q15: Is amoxicillin addictive?
Q16: Do I need a prescription for amoxicillin?
Q17: What are the long-term effects of amoxicillin?
Q18: What alternatives are available if I am allergic to amoxicillin?
Q19: How should I store amoxicillin?
Q20: What should I do if I have an allergic reaction to amoxicillin?
Q21: Can amoxicillin treat tooth infections?
Q22: Does amoxicillin treat viral infections like cold or flu?
Q23: Why isn’t amoxicillin working for my infection?
Q24: Can I stop taking amoxicillin early if I feel better?
Q25: Can children take amoxicillin?
Q26: Can elderly patients take amoxicillin?
Q27: Can diabetics take amoxicillin?
Q28: Can kidney patients take amoxicillin?
Q29: Can liver patients take amoxicillin?
Q30: Is amoxicillin the same as penicillin?
Q31: Does amoxicillin affect birth control pills?
Q32: Can I take amoxicillin if I’m allergic to sulfa?
Q33: What is the difference between amoxicillin and amoxicillin-clavulanate?
Q34: Can amoxicillin cause yeast infections?
Q35: Can I exercise while taking amoxicillin?
Q36: Does amoxicillin cause photosensitivity?
Q37: Can amoxicillin treat sinus infections?
Q38: Can amoxicillin treat UTIs?
Q39: Is generic amoxicillin as effective as brand-name?
Q40: Can I open an amoxicillin capsule?
Q41: Does amoxicillin cause constipation?
Q42: Can I take antacids with amoxicillin?
Q43: What is high-dose amoxicillin?
Q44: Can amoxicillin be used for acne?
Q45: Does amoxicillin stain teeth?
Q46: Is amoxicillin safe for pets?
Q47: Can amoxicillin treat bronchitis?
Q48: How should I dispose of unused amoxicillin?
Q49: Does amoxicillin cause depression or anxiety?
Q50: How long is a typical course of amoxicillin?
Q51: What is the difference between amoxicillin and ampicillin?
Amoxicillin stands as one of the most important antibiotics in modern medicine—a testament to rational drug design and decades of clinical evidence. From treating common childhood ear infections to eradicating H. pylori and preventing life-threatening endocarditis, its versatility is unmatched among oral antibiotics. Understanding its mechanism of action, spectrum, pharmacokinetics, and safety profile empowers both clinicians and patients to use this essential medicine responsibly and effectively.
We have journeyed through the complete pharmacodynamic and pharmacokinetic profile of amoxicillin, explored its clinical applications across multiple organ systems, addressed the critical issue of antibiotic resistance, and answered over 50 of the most commonly searched questions. For Urdu-speaking readers, we clarified اموکسیلن کیا ہے؟ and its clinical utility, ensuring language is no barrier to understanding this critical medication.
As with all medical sciences, this knowledge is intended to inform and educate. No article can replace the personalized judgment of a healthcare provider who weighs your unique physiology, genetics, and circumstances against the pharmacodynamic profile of a drug. That collaboration—between patient, provider, and the science of pharmacology—is where true healing begins.
References
1. Amoxicillin. Drugs and Lactation Database (LactMed), National Library of Medicine (US), 2023.
2. World Health Organization. Model List of Essential Medicines, 2023.
3. Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing, 33rd ed., 2023.
4. American Dental Association. Antibiotic Prophylaxis Prior to Dental Procedures, 2021.
5. Shulman ST, et al. Clinical Practice Guideline for the Diagnosis and Management of Group A Streptococcal Pharyngitis. Clin Infect Dis. 2012;55(10):e86–102.
6. Chow AW, et al. IDSA Clinical Practice Guideline for Acute Bacterial Rhinosinusitis in Children and Adults. Clin Infect Dis. 2012;54(8):e72–e112.
7. Lieberthal AS, et al. Clinical Practice Guideline: Otitis Media with Effusion. Pediatrics. 2016;137(6):e20162791.
8. Grayson ML, et al. Kucers’ The Use of Antibiotics, 7th ed., CRC Press, 2017.
9. U.S. Food and Drug Administration. Prescribing Information: Amoxil (amoxicillin), 2022.
10. European Medicines Agency. Amoxicillin Product Information, 2023.
11. SENTRY Antimicrobial Surveillance Program. In vitro activity of amoxicillin against respiratory pathogens, 2022.
12. Cochrane Database Syst Rev. Antibiotics for acute otitis media in children, 2023.
13. JAMA Pediatrics. Amoxicillin versus Amoxicillin-Clavulanate for Pediatric Sinusitis—Network Meta-analysis, 2024.
14. Brunton LL, Hilal-Dandan R, Knollmann BC, eds. Goodman & Gilman’s: The Pharmacological Basis of Therapeutics. 13th ed. McGraw-Hill; 2018.
15. Rang HP, Ritter JM, Flower RJ, Henderson G. Rang & Dale’s Pharmacology. 9th ed. Elsevier; 2020.
Last Updated: June 2026 | Version: 1.0 | Review Frequency: Annual review recommended
This article has been written with a focus on evidence-based medicine, clinical pharmacology, and practical application for medical students, residents, and practicing clinicians. The content aligns with contemporary antimicrobial stewardship principles and integrates the latest guidelines from WHO, IDSA, CDC, and ADA.
