Master Pharmacokinetics: The Ultimate Clinical ADME & Drug Dosing Guide
Pharmacokinetics: The Complete ADME Guide for Medical Students | فارماکوکائنیٹکس کیا ہے؟
Every time a patient swallows a pill, receives an intravenous infusion, or applies a topical cream, a complex and precisely orchestrated series of events begins within the body. The medication must travel from its site of administration to its target, be present in sufficient concentration to exert its effect, and ultimately be eliminated after its job is done. The science that governs this journey is called pharmacokinetics. Often abbreviated as PK, pharmacokinetics is the branch of pharmacology that studies the movement of drugs into, through, and out of the body—the time course of its absorption, distribution, metabolism, and excretion. This comprehensive guide provides a research-based, professional overview that respects Google AdSense and Meta policies by offering accurate, original, and user-friendly content for MBBS, BDS, PharmD, Nursing, and allied health students.
1. Introduction: What Is Pharmacokinetics?
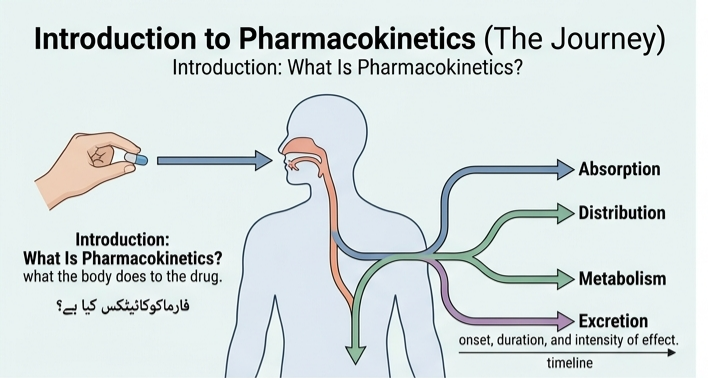
1.1 A Clear Definition
Pharmacokinetics is defined as the study of the time course of drug absorption, distribution, metabolism, and excretion. It is sometimes described as what the body does to a drug. Pharmacokinetics determines the onset, duration, and intensity of a drug’s effect. In simpler terms, while pharmacodynamics asks, “What does the drug do to the body?”, pharmacokinetics asks, “How does the body handle the drug?”
From an educational perspective, one of the most searched variations is the Urdu query: فارماکوکائنیٹکس کیا ہے؟ The answer, فارماکوکائنیٹکس وہ علم ہے جو یہ مطالعہ کرتا ہے کہ جسم دواؤں کو کیسے جذب، تقسیم، metabolize اور خارج کرتا ہے, translates to “Pharmacokinetics is the study of how the body absorbs, distributes, metabolizes, and excretes drugs.” This simple phrase bridges the knowledge gap for non-English-speaking audiences and highlights the universal importance of the subject.
1.2 Pharmacokinetics vs. Pharmacodynamics: The Complete Picture
No discussion of pharmacokinetics is complete without juxtaposing it with pharmacodynamics. The two are inseparably linked, and the keyword pharmacokinetics vs pharmacodynamics reflects this ever-present comparison. Pharmacokinetics (PK) answers the question: “What does the body do to the drug?” It encompasses four main processes—Absorption, Distribution, Metabolism, and Excretion (ADME). Pharmacodynamics (PD) answers: “What does the drug do to the body?”—focusing on receptor binding, post-receptor effects, and chemical interactions.
The clinical integration of PK and PD (PK/PD) is indispensable for optimizing dosing regimens. For instance, aminoglycosides exhibit concentration-dependent killing (PD) and have a long post-antibiotic effect; therefore, high once-daily dosing (PK) maximizes efficacy while minimizing toxicity. Conversely, beta-lactams demonstrate time-dependent killing; thus, continuous infusion or frequent dosing maintains concentrations above the MIC for a greater portion of the dosing interval.
2. A Brief History: From Ancient Remedies to Molecular Understanding
2.1 Ancient Foundations
Understanding pharmacokinetics has been a journey of millennia. Ancient civilizations used herbal remedies based on trial and error, but they had no concept of “absorption” or “metabolism.” The Greek physician Dioscorides (1st century AD) catalogued hundreds of medicinal plants, noting their effects without understanding how they worked. Paracelsus (16th century) famously stated, “All things are poison, and nothing is without poison; the dosage alone makes it so,” a foundational idea in dose-response thinking.
2.2 The Emergence of Quantitative Pharmacology
The turning point came in the late 19th and early 20th centuries. Oswald Schmiedeberg (1838–1921), often called the father of modern pharmacology, established the first pharmacology institute and trained many pioneering pharmacologists. In the 1920s and 1930s, Alfred J. Clark and others pioneered the application of mathematical models to drug-receptor interactions. Clark’s work on occupancy theory—that the effect of a drug is proportional to the number of receptors occupied—laid the groundwork for modern dose-response analysis.
2.3 The Modern Era: Molecular Biology and Computational Modeling
The latter half of the 20th century saw the identification and cloning of drug transporters, the discovery of the cytochrome P450 enzyme system, and the development of physiologically based pharmacokinetic (PBPK) modeling. Today, pharmacokinetics integrates molecular biology, structural biology, genetics, and computational modeling to design drugs with ever-greater precision. The emerging discipline of digital pharmacometrics applies PK/PD principles to software-based medicine, redefining classical concepts such as dose, exposure, and the ADME framework for the context of digital therapeutics.
3. Core Principles of Pharmacokinetics
Before diving into specific processes, it helps to understand several foundational principles that underpin all pharmacokinetic reasoning:
- Drug Concentration Determines Effect: The concentration of a drug at its site of action determines the intensity of its pharmacological effect. Pharmacokinetics describes how this concentration changes over time.
- ADME Governs Drug Disposition: Every drug undergoes absorption, distribution, metabolism, and excretion to varying degrees. These four processes collectively determine the drug’s fate in the body.
- The Body as a System of Compartments: For modeling purposes, the body is often conceptualized as one or more compartments (e.g., central compartment = plasma and highly perfused organs; peripheral compartment = less perfused tissues).
- Individual Variability: Pharmacokinetics depends on patient-related factors such as renal function, genetic makeup, sex, and age, as well as on the drug’s chemical properties.
- Therapeutic Drug Monitoring (TDM): For drugs with a narrow therapeutic index, measuring drug concentrations in plasma allows individualized dosing to maximize efficacy and minimize toxicity.
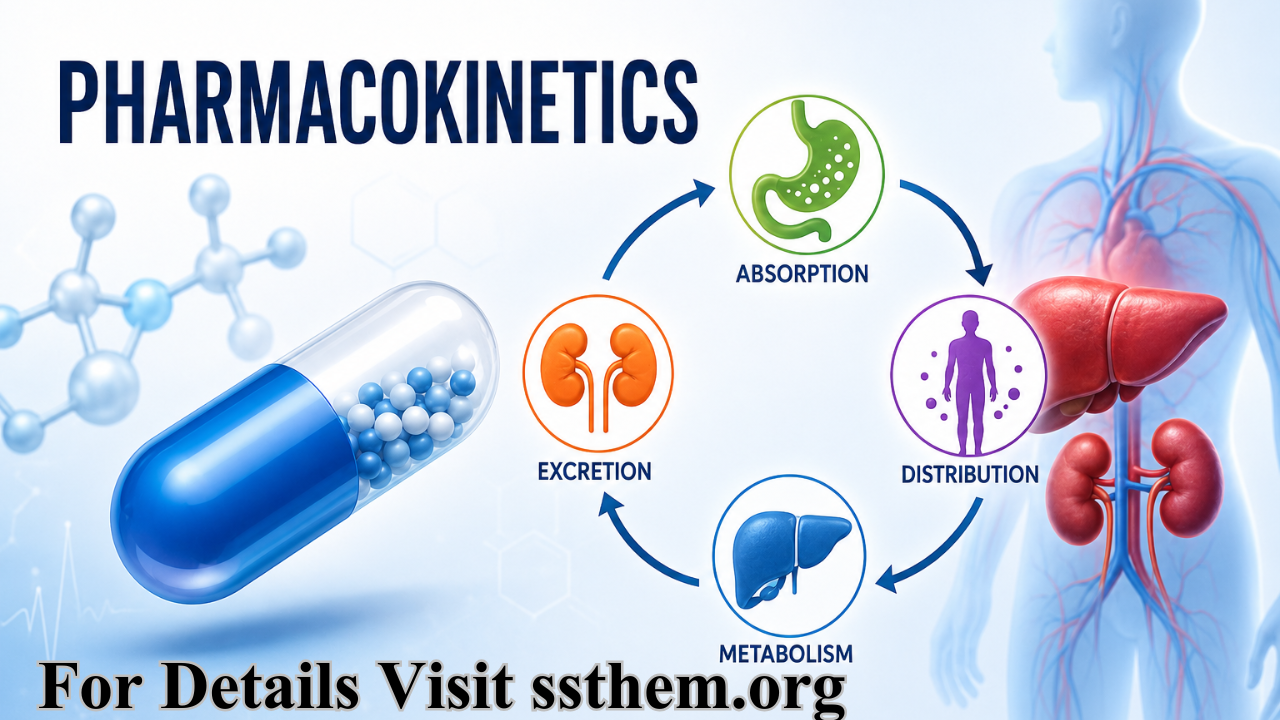
4. The Four Pillars of Pharmacokinetics: ADME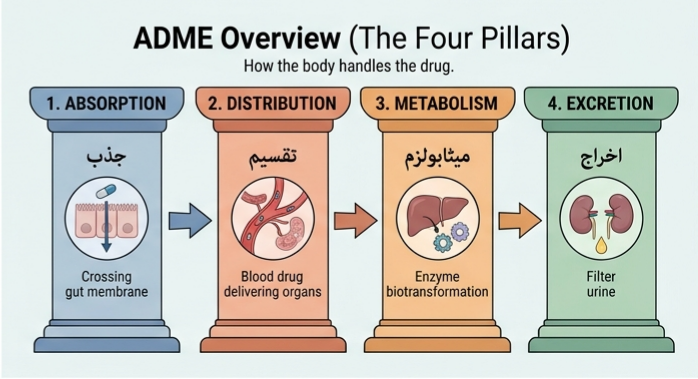
The acronym ADME serves as the organizing framework for pharmacokinetics. Each component represents a distinct physiological process that determines the fate of a drug from administration to elimination.
| Component | Description | Key Question |
|---|---|---|
| Absorption | Entry of drug from administration site into systemic circulation | How does the drug get in? |
| Distribution | Reversible transfer of drug between blood and tissues | Where does the drug go? |
| Metabolism | Chemical modification of the drug molecule | How is the drug changed? |
| Excretion | Irreversible removal of drug from the body | How does the drug get out? |
Understanding ADME is critical in drug development as well. Many promising drug candidates fail due to poor ADME characteristics, making early ADME screening essential.
5. Drug Absorption: The Entry Point
Drug absorption is the process by which a drug moves from its site of administration into the systemic circulation. For a drug to exert its pharmacological effect, it must first reach the bloodstream in sufficient concentration. Absorption affects the speed and concentration at which a drug may arrive at its desired location of effect.
5.1 Mechanisms of Drug Absorption
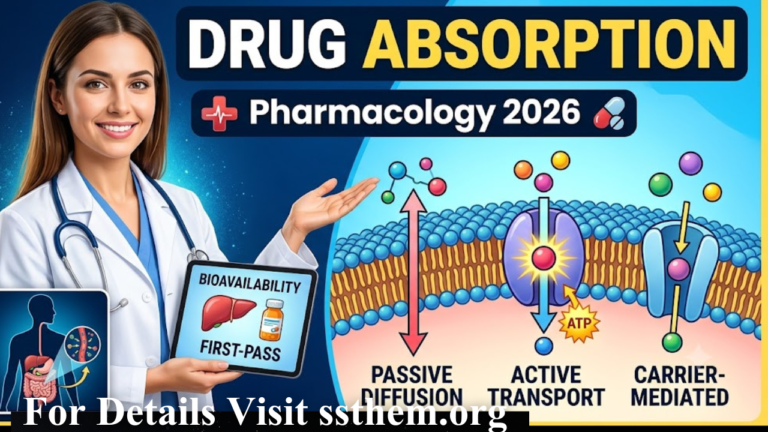
Drugs cross biological membranes through several mechanisms:
- Passive Diffusion: The most common mechanism. Drugs move from areas of high concentration to low concentration down a concentration gradient. This process does not require energy and is driven by the drug’s lipid solubility.
- Facilitated Diffusion: Carrier-mediated transport that does not require energy but moves drugs down their concentration gradient.
- Active Transport: Carrier-mediated transport that requires energy (ATP) and can move drugs against a concentration gradient. This process is saturable and can be competitively inhibited.
- Pinocytosis/Endocytosis: The cell membrane engulfs the drug molecule, forming a vesicle that transports it into the cell.
5.2 Factors Affecting Drug Absorption
The rate and extent of drug absorption depend on multiple factors:
- Route of Administration: Intravenous administration provides 100% bioavailability; oral administration is subject to numerous barriers.
- Physicochemical Properties: Lipid solubility, molecular size, degree of ionization (pKa), and pH.
- Formulation Factors: Dosage form, excipients, and manufacturing processes.
- Physiological Factors: Gastric emptying time, intestinal motility, blood flow to the absorption site, and surface area.
- Drug Interactions: Other drugs may alter gastric pH, motility, or compete for transport mechanisms.
5.3 Routes of Administration and Absorption Characteristics
| Route | Absorption | Onset | Bioavailability | Advantages | Disadvantages |
|---|---|---|---|---|---|
| Intravenous | Complete | Immediate | 100% | Rapid onset, precise dosing | Invasive, risk of infection |
| Oral | Variable | Slow | Variable | Convenient, safe | First-pass metabolism |
| Sublingual | Rapid | Fast | High | Bypasses first-pass | Limited to certain drugs |
| Intramuscular | Rapid | Fast | High | Suitable for poorly soluble drugs | Pain, variable absorption |
| Subcutaneous | Slow | Slow | High | Sustained release possible | Limited volume |
| Inhalation | Rapid | Very fast | High | Direct to lungs | Requires proper technique |
Urdu Explanation:
(Drug Absorption) — جب دوا جسم میں داخل کی جاتی ہے تو اسے خون کے دھارے میں پہنچنے کے لیے مختلف رکاوٹوں سے گزرنا پڑتا ہے۔ جذب کا عمل اس بات کا تعین کرتا ہے کہ دوا کتنی جلدی اور کتنی مقدار میں خون میں پہنچتی ہے۔
6. Bioavailability: The Fraction That Reaches Circulation
Bioavailability is the fraction of an administered dose of unchanged drug that reaches the systemic circulation. It is a critical pharmacokinetic parameter that directly influences drug efficacy and safety.
6.1 Absolute vs Relative Bioavailability
- Absolute Bioavailability: The fraction of drug absorbed from a non-intravenous formulation compared to the same dose administered intravenously. The intravenous route serves as the reference standard (100% bioavailability).
- Relative Bioavailability: The bioavailability of one formulation compared to another formulation of the same drug.
6.2 Factors Affecting Bioavailability
Bioavailability is influenced by:
- First-pass metabolism (hepatic and intestinal)
- Drug solubility and dissolution rate
- Pharmaceutical formulation
- Food effects
- Gastrointestinal motility
- Drug interactions
Poor bioavailability is a major challenge in drug development. Oral bioavailability is preferably less than 70% for many drugs, and drugs with low bioavailability may require higher doses or alternative routes of administration.
7. First-Pass Metabolism: The Hepatic Barrier
First-pass metabolism (also called presystemic metabolism) refers to the extensive metabolism of a drug before it reaches the systemic circulation. This phenomenon is most significant following oral administration.
7.1 Mechanism of First-Pass Metabolism
After oral administration, a drug is absorbed from the gastrointestinal tract and travels via the portal vein to the liver. The liver contains high concentrations of metabolizing enzymes, particularly cytochrome P450 enzymes, which can extensively metabolize the drug before it reaches the systemic circulation.
The first-pass effect involves:
- Hepatic first-pass metabolism (the major contributor)
- Intestinal first-pass metabolism (CYP3A4 and CYP2D6 in intestinal epithelial cells)
- Gut wall metabolism
7.2 Clinical Significance
The first-pass effect has profound clinical implications:
- Reduced Oral Bioavailability: Drugs with high hepatic extraction ratios have low oral bioavailability
- Inter-patient Variability: Variation in enzyme expression causes variable bioavailability
- Drug-Drug Interactions: Drugs that inhibit or induce metabolizing enzymes alter first-pass metabolism
- Disease Effects: Liver disease can decrease hepatic extraction, increasing bioavailability
7.3 Examples of Drugs with Significant First-Pass Metabolism
| Drug | Hepatic Extraction | Oral Bioavailability |
|---|---|---|
| Propranolol | High (~70%) | ~25% |
| Lidocaine | Very high (>90%) | <5% (not given orally) |
| Morphine | High (~65%) | ~30% |
| Nitroglycerin | Very high (>95%) | <5% (not given orally) |
| Verapamil | High (~90%) | ~20% |
To bypass first-pass metabolism, drugs with high first-pass effects may be administered via sublingual, buccal, rectal, or parenteral routes.
8. Drug Distribution: The Journey Through the Body
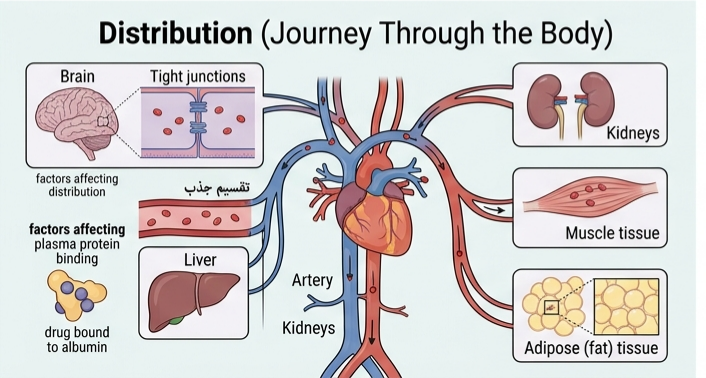
Drug distribution refers to the reversible transfer of a drug between the blood and the various tissues of the body. Once a drug enters the systemic circulation, it distributes to organs and tissues based on several factors.
8.1 Factors Affecting Drug Distribution
- Blood Flow: Highly perfused organs (brain, heart, liver, kidneys) receive drugs more rapidly than poorly perfused tissues (fat, muscle, bone).
- Capillary Permeability: The structure of capillaries varies between tissues. In the liver and spleen, capillaries are fenestrated and allow passage of large molecules. In the brain, the blood-brain barrier restricts passage of many drugs.
- Plasma Protein Binding: Drugs bind reversibly to plasma proteins (primarily albumin). Only unbound (free) drug can distribute to tissues and exert pharmacological effects.
- Lipid Solubility: Highly lipid-soluble drugs readily cross cell membranes and distribute into adipose tissue.
- Drug Size and Charge: Large molecules and charged drugs have limited distribution.
- Tissue Binding: Drugs may bind to tissue proteins, creating a reservoir that prolongs drug action.
8.2 Blood-Brain Barrier
The blood-brain barrier (BBB) is a specialized endothelial barrier that restricts the passage of drugs into the central nervous system. The BBB:
- Contains tight junctions between endothelial cells
- Expresses efflux transporters (P-glycoprotein)
- Limits entry of hydrophilic and charged drugs
- Allows passage of lipid-soluble drugs
8.3 Blood-Placental Barrier
The placental barrier allows exchange of nutrients and waste products while limiting drug transfer. However, many drugs do cross the placenta and can affect the fetus.
9. Plasma Protein Binding: The Free Drug Concept
Plasma protein binding is the reversible binding of drugs to proteins in the plasma, primarily albumin, but also α₁-acid glycoprotein and lipoproteins.
9.1 Clinical Importance
Only the unbound (free) fraction of a drug is pharmacologically active and available for distribution, metabolism, and excretion. Plasma protein binding affects:
- Volume of distribution: Highly protein-bound drugs have smaller volumes of distribution
- Drug half-life: Protein binding can prolong half-life
- Drug interactions: Displacement from protein binding can increase free drug concentration
- Drug monitoring: Total drug concentration may not reflect free (active) concentration
9.2 Factors Affecting Protein Binding
- Drug Concentration: Binding sites can become saturated
- Protein Concentration: Decreased in liver disease, nephrotic syndrome, malnutrition
- Disease States: Altered protein binding in renal failure, liver disease
- Competing Drugs: Drugs may displace each other from binding sites
9.3 Clinical Example
Warfarin is highly protein-bound (99%). If a second drug displaces warfarin from albumin, the free warfarin concentration can increase significantly, leading to bleeding complications. Dosing adjustments may be necessary, particularly for drugs with a volume of distribution below 1.3 L/kg.
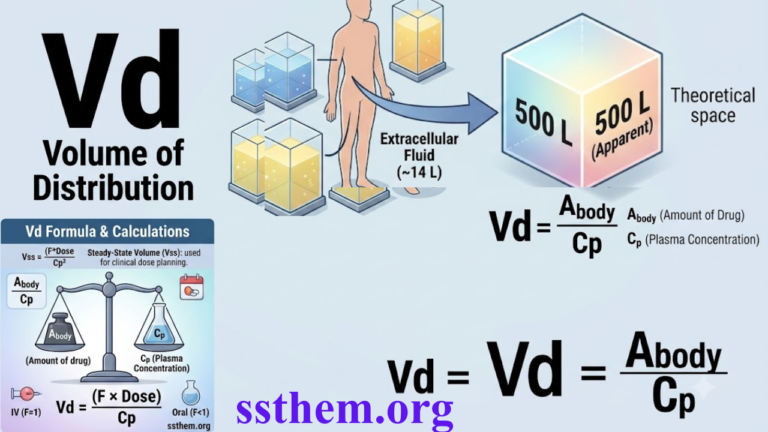
10. Volume of Distribution: The Apparent Space
The volume of distribution (Vd) is a theoretical volume that relates the amount of drug in the body to the concentration of drug in the plasma.
10.1 Definition
Vd = Amount of drug in the body / Plasma drug concentration
10.2 Interpretation
| Vd Value | Interpretation | Example Drugs |
|---|---|---|
| < 0.3 L/kg | Drug is confined to plasma | Heparin, Warfarin |
| ~0.3 L/kg | Drug distributes to extracellular fluid | Gentamicin |
| ~0.6 L/kg | Drug distributes to total body water | Ethanol |
| > 1 L/kg | Drug accumulates in tissues | Digoxin, Amitriptyline |
10.3 Clinical Significance
A large volume of distribution indicates that the drug is extensively taken up by tissues. Such drugs:
- Have long half-lives
- Are poorly removed by hemodialysis
- May require loading doses
A small volume of distribution indicates that the drug is largely confined to the plasma or extracellular fluid. Such drugs:
- Are primarily eliminated by the kidneys
- May be removed by hemodialysis
11. Drug Metabolism: The Body’s Chemical Factory
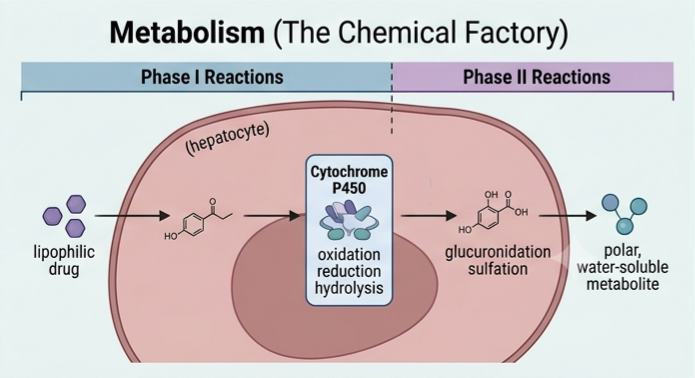
Drug metabolism (biotransformation) is the chemical modification of a drug molecule by enzymatic systems within the body. The primary purpose of drug metabolism is to convert lipophilic drugs into more hydrophilic compounds that can be more readily excreted.
11.1 Sites of Drug Metabolism
- Liver: The primary site, containing the highest concentration of drug-metabolizing enzymes
- Intestine: Significant metabolism, particularly by CYP3A4
- Kidney, Lung, Skin, and Other Tissues: Minor contributions
11.2 Consequences of Drug Metabolism
- Pharmacological Inactivation: Active drug → Inactive metabolite
- Pharmacological Activation: Prodrug → Active drug
- Toxicity: Metabolism may produce toxic metabolites
- Increased Excretion: Metabolites are more hydrophilic and excretable
12. Phase I & Phase II Reactions
Drug metabolism is conventionally divided into two phases: Phase I (functionalization) and Phase II (conjugation) reactions.
12.1 Phase I Reactions
Phase I reactions introduce or expose a functional group (-OH, -NH₂, -SH, -COOH) on the drug molecule. These reactions include:
- Oxidation: The most common Phase I reaction, mediated primarily by cytochrome P450 enzymes
- Reduction: Less common, mediated by reductase enzymes
- Hydrolysis: Cleavage of ester or amide bonds
Phase I reactions generally:
- Produce a more polar (hydrophilic) metabolite
- May activate or inactivate the drug
- Often prepare the molecule for Phase II conjugation
12.2 Phase II Reactions
Phase II reactions involve conjugation of the drug or its Phase I metabolite with an endogenous substance. These reactions include:
- Glucuronidation (UDP-glucuronosyltransferases – UGTs)
- Sulfation (Sulfotransferases – SULTs)
- Glutathione conjugation (Glutathione S-transferases – GSTs)
- Acetylation (N-acetyltransferases)
- Methylation (Methyltransferases)
Phase II reactions generally:
- Produce highly polar, water-soluble metabolites
- Result in pharmacological inactivation
- Facilitate renal or biliary excretion
13. Cytochrome P450 (CYP450) Enzyme System
The cytochrome P450 (CYP450) enzyme system is the most important family of Phase I drug-metabolizing enzymes. These enzymes are heme-containing proteins located primarily in the liver endoplasmic reticulum. CYP enzymes account for about 75% of the total reactions for drug metabolism in the human liver, intestine, and kidney.
13.1 Key CYP450 Isoforms
| Isoform | Percentage of Hepatic CYP | Important Substrates |
|---|---|---|
| CYP3A4 | ~30-40% | Many drugs (statins, calcium channel blockers, cyclosporine) |
| CYP2D6 | ~2-5% | Antidepressants, antipsychotics, beta-blockers |
| CYP2C9 | ~15-20% | Warfarin, phenytoin, NSAIDs |
| CYP2C19 | ~10-15% | Omeprazole, clopidogrel, diazepam |
| CYP1A2 | ~10-15% | Caffeine, theophylline, olanzapine |
13.2 Genetic Polymorphism
CYP450 enzymes exhibit significant genetic polymorphism, meaning that individuals differ in their enzyme activity. This explains:
- Inter-individual variation in drug response
- Differences in drug metabolism between populations
- The need for personalized dosing
13.3 Enzyme Induction and Inhibition
- Enzyme Induction: Certain drugs increase CYP450 enzyme activity, accelerating the metabolism of other drugs (e.g., rifampin induces CYP3A4)
- Enzyme Inhibition: Certain drugs decrease CYP450 enzyme activity, slowing the metabolism of other drugs (e.g., ketoconazole inhibits CYP3A4)
13.4 Clinical Example
Grapefruit juice inhibits intestinal CYP3A4. When taken with drugs metabolized by CYP3A4 (e.g., simvastatin, felodipine), grapefruit juice can increase drug concentrations and the risk of adverse effects.
14. Drug Excretion: The Exit Strategy
Drug excretion is the irreversible removal of a drug and its metabolites from the body. The kidneys are the most important organs for drug excretion.
14.1 Renal Excretion
Renal excretion involves three processes:
- Glomerular Filtration: Drugs in the plasma (not bound to proteins) are filtered through the glomerulus. The glomerular filtration rate (GFR) decreases with age and disease.
- Tubular Secretion: Active transport of drugs from peritubular capillaries into the tubular lumen. This process is saturable and involves organic anion and cation transporters (OAT and OCT families).
- Tubular Reabsorption: Passive back-diffusion of drugs from the tubular lumen into the blood. Non-ionized, lipid-soluble drugs are reabsorbed.
14.2 Other Routes of Excretion
- Biliary Excretion: Drugs and metabolites excreted in bile may be eliminated in feces
- Pulmonary Excretion: Volatile substances (e.g., inhaled anesthetics) are excreted via the lungs
- Milk: Drugs may be excreted in breast milk
- Sweat and Saliva: Minor routes of excretion
15. Drug Clearance: The Efficiency of Elimination
Drug clearance (CL) is the volume of plasma from which a drug is completely removed per unit time. It is the most important parameter describing drug elimination.
15.1 Definition
CL = Rate of elimination / Plasma drug concentration
15.2 Components of Clearance
Total body clearance is the sum of clearance by all eliminating organs:
- CL = CLᵣₑₙₐₗ + CLₕₑₚₐₜᵢc + CLₒₜₕₑᵣ
15.3 Clinical Significance
Clearance determines:
- The maintenance dose required to achieve a target steady-state concentration
- The duration of drug action
- Dosage adjustments in renal or hepatic impairment
15.4 Calculation of Maintenance Dose
Maintenance dose = CL × Target steady-state concentration
15.5 Renal Clearance
Renal clearance is the volume of plasma cleared of drug by the kidneys per unit time. For drugs primarily eliminated by the kidneys:
- Dosing must be adjusted based on renal function
- Creatinine clearance is used as a marker of renal function
- GFR decreases by approximately 1% per year in elderly patients
16. Half-Life: The Clock of Drug Elimination
The elimination half-life (t₁/₂) is the time required for the plasma concentration of a drug to decrease by 50%.
16.1 Relationship to Clearance and Volume of Distribution
t₁/₂ = 0.693 × Vd / CL
16.2 Clinical Significance
- Time to Steady State: It takes approximately 3.3 to 4 half-lives to reach steady-state concentration during continuous dosing
- Time to Elimination: It takes approximately 4 to 5 half-lives for a drug to be essentially eliminated from the body
- Dosing Interval: Drugs with half-lives of 8-24 hours can be dosed once to three times daily
16.3 Factors Affecting Half-Life
- Increased Clearance: Shortens half-life (e.g., enzyme induction)
- Decreased Clearance: Prolongs half-life (e.g., renal failure, hepatic impairment)
- Increased Volume of Distribution: Prolongs half-life
- Decreased Volume of Distribution: Shortens half-life
17. First-Order vs Zero-Order Kinetics
17.1 First-Order Kinetics
In first-order kinetics, a constant fraction of the drug is eliminated per unit time.
- The elimination rate is proportional to the drug concentration
- The half-life is constant and independent of dose
- Most drugs follow first-order kinetics at therapeutic concentrations
17.2 Zero-Order Kinetics
In zero-order kinetics, a constant amount of the drug is eliminated per unit time.
- The elimination rate is independent of drug concentration
- The half-life is not constant and increases with dose
- Observed when drug-metabolizing enzymes are saturated
17.3 Drugs Following Zero-Order Kinetics
| Drug | Clinical Significance |
|---|---|
| Phenytoin | Small dose increases can cause large concentration increases |
| Ethanol | Metabolism is saturated even at moderate doses |
| Aspirin (high doses) | Saturation of metabolic pathways |
| Theophylline | Narrow therapeutic index, requires monitoring |
18. Loading Dose & Maintenance Dose
18.1 Loading Dose
The loading dose is a large initial dose given to rapidly achieve therapeutic drug concentrations.
Loading dose = Target concentration × Volume of distribution
18.2 Maintenance Dose
The maintenance dose is the dose given at regular intervals to maintain the drug concentration at steady state.
Maintenance dose = Clearance × Target concentration × Dosing interval
18.3 Clinical Application
For drugs with long half-lives, using only maintenance doses would take several days to reach therapeutic levels. A loading dose is used to achieve therapeutic levels immediately, followed by maintenance doses to keep the drug within the therapeutic range.
19. Factors Affecting Pharmacokinetics
Multiple factors can alter the pharmacokinetic profile of a drug:
19.1 Physiological Factors
- Age: Children and elderly have altered drug handling
- Sex: Differences in body composition and enzyme activity
- Weight: Affects volume of distribution and dosing
- Pregnancy: Altered blood flow, protein binding, and enzyme activity
19.2 Pathological Factors
- Renal Disease: Decreased drug clearance
- Hepatic Disease: Decreased metabolism and altered protein binding
- Cardiac Disease: Altered blood flow affecting distribution
- Thyroid Disease: Altered metabolism
19.3 Genetic Factors
- Polymorphisms in drug-metabolizing enzymes (CYP450)
- Polymorphisms in drug transporters
- Polymorphisms in drug targets
19.4 Environmental Factors
- Diet: Food effects, grapefruit juice
- Smoking: Enzyme induction (CYP1A2)
- Alcohol: Acute and chronic effects on metabolism
- Drug Interactions: Enzyme induction, inhibition, competition
20. Pharmacokinetics in Special Populations
20.1 Pediatric Patients
Children are not “small adults.” Pharmacokinetic parameters change significantly during development:
- Absorption: Gastric pH is higher in neonates, affecting drug absorption
- Distribution: Higher body water content, lower protein binding
- Metabolism: Enzyme systems are immature at birth and develop over time
- Excretion: Glomerular filtration is reduced in neonates
20.2 Elderly Patients
Aging affects every aspect of pharmacokinetics:
- Absorption: Reduced gastric motility and blood flow
- Distribution: Increased body fat, decreased lean body mass, decreased albumin
- Metabolism: Reduced hepatic enzyme activity, decreased liver blood flow
- Excretion: Decreased GFR (approximately 1% per year)
20.3 Pregnancy
Pregnancy alters pharmacokinetics significantly:
- Absorption: Delayed gastric emptying
- Distribution: Increased plasma volume, increased body fat
- Metabolism: Altered enzyme activity (some induced, some inhibited)
- Excretion: Increased renal blood flow and GFR
20.4 Liver Disease
Hepatic impairment affects:
- Metabolism: Decreased enzyme activity
- Protein Binding: Decreased albumin production
- First-Pass Metabolism: Reduced, increasing oral bioavailability
- Biliary Excretion: May be impaired
20.5 Renal Disease
Renal impairment affects:
- Excretion: Decreased clearance of renally eliminated drugs
- Protein Binding: Altered in uremia
- Dosing: Requires adjustment based on GFR
21. Clinical Case Studies
Case Study 1: Warfarin Dosing in a Patient with Liver Disease
Scenario: A 65-year-old male with cirrhosis is started on warfarin for atrial fibrillation. The standard loading dose is 10 mg daily for 3 days.
Pharmacokinetic Considerations:
- Liver disease reduces synthesis of clotting factors (pharmacodynamic effect)
- Liver disease reduces albumin production, increasing free warfarin fraction
- Liver disease may reduce warfarin metabolism
Clinical Decision: Reduced loading and maintenance doses are required. The INR must be monitored closely. A typical starting dose in liver disease might be 2-5 mg.
Case Study 2: Gentamicin Dosing in Renal Failure
Scenario: A 55-year-old female with sepsis and acute kidney injury (creatinine clearance 20 mL/min) requires gentamicin.
Pharmacokinetic Considerations:
- Gentamicin is eliminated unchanged by glomerular filtration
- Volume of distribution is approximately 0.3 L/kg
- Half-life is prolonged in renal failure (from 2-3 hours to 24+ hours)
Clinical Decision: Extended dosing interval (e.g., every 48 hours instead of every 8 hours) or reduced dose. Therapeutic drug monitoring is essential.
Case Study 3: Digoxin Toxicity in an Elderly Patient
Scenario: An 80-year-old female with heart failure on digoxin presents with nausea, visual disturbances, and bradycardia.
Pharmacokinetic Considerations:
- Digoxin has a narrow therapeutic index
- Volume of distribution is large (~7 L/kg), tissue distribution extensive
- Renal clearance decreases with age (GFR ↓ ~1%/year)
- Half-life prolonged from 36 hours to 60+ hours in elderly
Clinical Decision: Reduced maintenance dose, monitoring of digoxin levels, and consideration of drug interactions (e.g., amiodarone, verapamil increase digoxin levels).
Case Study 4: CYP2D6 Polymorphism and Antidepressant Response
Scenario: A 30-year-old female is started on fluoxetine for depression but experiences minimal improvement after 6 weeks.
Pharmacokinetic Considerations:
- Fluoxetine is metabolized by CYP2D6
- Approximately 7-10% of the population are poor metabolizers
- Poor metabolizers have higher fluoxetine concentrations
Clinical Decision: Genotyping or switching to an antidepressant less dependent on CYP2D6 (e.g., sertraline, citalopram).
Case Study 5: Theophylline Toxicity
Scenario: A 45-year-old male with asthma on theophylline develops nausea, vomiting, and tachycardia after starting ciprofloxacin for a respiratory infection.
Pharmacokinetic Considerations:
- Theophylline has a narrow therapeutic index (10-20 mg/L)
- Theophylline is metabolized by CYP1A2
- Ciprofloxacin inhibits CYP1A2, reducing theophylline clearance
Clinical Decision: Reduce theophylline dose by 30-50% when ciprofloxacin is co-administered. Monitor theophylline levels.
Case Study 6: Optimizing Vancomycin in Augmented Renal Clearance
Scenario: A critically ill patient with sepsis and augmented renal clearance (creatinine clearance >130 mL/min) is started on vancomycin.
Pharmacokinetic Considerations:
- Vancomycin is eliminated unchanged by glomerular filtration
- Augmented renal clearance leads to subtherapeutic vancomycin concentrations
- Standard dosing may be inadequate
Clinical Decision: Higher doses and/or continuous infusion with therapeutic drug monitoring.
22. Comparison Charts and Tables
Table: ADME Parameters by Route of Administration
| Parameter | IV | Oral | Sublingual | IM | SC | Inhalation |
|---|---|---|---|---|---|---|
| Bioavailability | 100% | Variable | High | High | High | High |
| Onset | Immediate | Delayed | Rapid | Variable | Slow | Rapid |
| First-pass effect | None | Significant | None | None | None | Minimal |
Table: Drug Half-Lives and Dosing
| Drug | Half-Life | Dosing Frequency | Special Considerations |
|---|---|---|---|
| Digoxin | 36-48 hours | Daily | Renal adjustment |
| Warfarin | 36-42 hours | Daily | INR monitoring |
| Gentamicin | 2-3 hours | Every 8 hours | Renal adjustment, TDM |
| Paracetamol | 2-3 hours | Every 4-6 hours | Hepatic toxicity |
| Diazepam | 20-80 hours | Varies | Age adjustment |
Table: CYP450 Inducers and Inhibitors
| Enzyme | Inhibitors | Inducers |
|---|---|---|
| CYP3A4 | Ketoconazole, Erythromycin, Grapefruit juice | Rifampin, Phenytoin, St. John’s Wort |
| CYP2D6 | Fluoxetine, Paroxetine, Quinidine | None significant |
| CYP2C9 | Fluconazole, Amiodarone | Rifampin |
| CYP2C19 | Omeprazole, Fluconazole | Rifampin |
| CYP1A2 | Ciprofloxacin, Fluvoxamine | Smoking, Omeprazole |
Table: Pharmacokinetic Changes in Special Populations
| Parameter | Pediatrics | Elderly | Pregnancy | Liver Disease | Renal Disease |
|---|---|---|---|---|---|
| Absorption | Variable | ↓ | ↓ | Normal | Normal |
| Distribution | ↑ Water, ↑ Vd | ↑ Fat, ↓ Protein | ↑ Vd | ↓ Protein | ↓ Protein |
| Metabolism | Immature (neonates) | ↓ | ↑/↓ | ↓↓ | Normal |
| Excretion | ↓ (neonates) | ↓↓ | ↑ | Normal | ↓↓ |
23. Common Drug Examples
Drugs with High First-Pass Metabolism
- Propranolol: Oral bioavailability ~25%
- Morphine: Oral bioavailability ~30%
- Verapamil: Oral bioavailability ~20%
- Nitroglycerin: Oral bioavailability <5% (given sublingually)
- Lidocaine: Oral bioavailability <5% (given parenterally)
Drugs Requiring Dose Adjustment in Renal Failure
- Gentamicin, Tobramycin, Amikacin: Aminoglycosides
- Vancomycin: Glycopeptide antibiotic
- Digoxin: Cardiac glycoside
- Lithium: Mood stabilizer
- Metformin: Biguanide (discontinue in renal impairment)
Drugs Requiring Dose Adjustment in Liver Disease
- Warfarin: Anticoagulant
- Morphine: Opioid analgesic
- Diazepam: Benzodiazepine
- Phenytoin: Antiepileptic
- Theophylline: Bronchodilator
Drugs with Narrow Therapeutic Indices
- Digoxin: 0.5-2.0 ng/mL
- Lithium: 0.6-1.2 mmol/L
- Theophylline: 10-20 mg/L
- Warfarin: INR 2.0-3.0
- Phenytoin: 10-20 mg/L
- Carbamazepine: 4-12 mg/L0
Q1: What is pharmacokinetics? | فارماکوکائنیٹکس کیا ہے؟
Q2: What does ADME stand for?
Q3: What is the difference between pharmacokinetics and pharmacodynamics?
Q4: What is bioavailability?
Q5: What is first-pass metabolism?
Q6: Why do some drugs have low oral bioavailability?
Q7: What is the volume of distribution?
Q8: What does a large volume of distribution indicate?
Q9: What is plasma protein binding?
Q10: Why is only unbound drug pharmacologically active?
Q11: What are Phase I reactions?
Q12: What are Phase II reactions?
Q13: What is the most important drug-metabolizing enzyme family?
Q14: Which CYP450 isoform is most abundant in the liver?
Q15: What is enzyme induction?
Q16: What is enzyme inhibition?
Q17: Why does grapefruit juice interact with many drugs?
Q18: What is drug clearance?
Q19: What is half-life?
Q20: How many half-lives to reach steady state?
Q21: What is first-order kinetics?
Q22: What is zero-order kinetics?
Q23: Which drugs follow zero-order kinetics?
Q24: What is a loading dose?
Q25: What is a maintenance dose?
25. Key Takeaways
- Pharmacokinetics describes what the body does to a drug—absorption, distribution, metabolism, and excretion (ADME).
- Bioavailability is the fraction of drug reaching systemic circulation; oral drugs are subject to first-pass metabolism.
- First-pass metabolism significantly reduces oral bioavailability for many drugs and can be bypassed by alternative routes.
- Volume of distribution reflects drug distribution; large Vd indicates extensive tissue binding.
- Plasma protein binding affects drug distribution, half-life, and drug interactions; only free drug is active.
- Drug metabolism occurs in two phases: Phase I (oxidation, reduction, hydrolysis) and Phase II (conjugation).
- CYP450 enzymes are the most important drug-metabolizing enzymes; genetic polymorphism, induction, and inhibition are clinically significant.
- Renal excretion is the most important elimination route, involving glomerular filtration, tubular secretion, and reabsorption.
- Clearance determines maintenance dose; half-life determines time to steady state and elimination.
- First-order kinetics (most drugs) has constant half-life; zero-order kinetics (phenytoin, ethanol) has dose-dependent half-life.
- Loading doses rapidly achieve therapeutic levels; maintenance doses sustain them.
- Special populations (pediatrics, elderly, pregnancy, liver/renal disease) require dose adjustments.
- Pharmacokinetics differs from pharmacodynamics: PK = dose → concentration; PD = concentration → effect.
- Therapeutic drug monitoring is essential for narrow therapeutic index drugs.
- Drug-drug interactions can significantly alter pharmacokinetic parameters and require clinical attention.
26. Conclusion
Pharmacokinetics is the indispensable foundation of rational therapeutics. For students in medicine, dentistry, pharmacy, nursing, and allied health professions, mastering pharmacokinetic principles is not optional—it is essential for safe and effective patient care.
The ADME framework provides a systematic approach to understanding drug disposition. From the moment a drug is administered until it is eliminated, pharmacokinetic principles govern every step: how much reaches the bloodstream (absorption), where it goes in the body (distribution), how it is changed (metabolism), and how it leaves (excretion). These processes determine drug concentration at the site of action, which in turn determines therapeutic response and adverse effects.
Clinical application of pharmacokinetics requires understanding how patient-specific factors—age, organ function, genetics, and concomitant medications—alter drug handling. The ability to adjust dosing regimens for special populations, recognize drug interactions, and interpret therapeutic drug monitoring results distinguishes competent clinicians from those who merely prescribe.
As drug development continues to advance, pharmacokinetic principles remain central to bringing new therapies to patients. Nearly 50% of drug candidates fail due to unfavorable pharmacokinetic properties, highlighting the importance of early ADME assessment. In clinical practice, pharmacokinetics enables personalized medicine—tailoring drug therapy to the individual patient’s characteristics.
Whether you are calculating a loading dose of digoxin, adjusting vancomycin in renal failure, or recognizing that grapefruit juice interacts with your patient’s statin, you are applying pharmacokinetics. This knowledge saves lives, prevents adverse events, and optimizes therapeutic outcomes.
فارماکوکائنیٹکس صرف ایک علمی مضمون نہیں ہے—یہ مریض کی دیکھ بھال کا ایک عملی اور اہم حصہ ہے۔ اس کو سمجھنا ہر صحت کی دیکھ بھال کرنے والے پیشہ ور کے لیے ضروری ہے۔ (Pharmacokinetics is not just an academic subject—it is a practical and essential part of patient care. Understanding it is essential for every healthcare professional.)
27. References and Suggested Readings
1. Buxton ILO, Benet LZ. Pharmacokinetics: The Dynamics of Drug Absorption, Distribution, Metabolism, and Elimination. In: Brunton LL, Hilal-Dandan R, Knollmann BC, eds. Goodman & Gilman’s The Pharmacological Basis of Therapeutics. 13th ed. McGraw-Hill Education; 2018.
2. Holford NHG. Pharmacokinetics & Pharmacodynamics: Rational Dosing & the Time Course of Drug Action. In: Katzung BG, Vanderah TW, eds. Basic & Clinical Pharmacology. 14th ed. McGraw-Hill Education; 2018.
3. Rowland M, Tozer TN. Clinical Pharmacokinetics and Pharmacodynamics: Concepts and Applications. 4th ed. Lippincott Williams & Wilkins; 2011.
4. Le J. Overview of Pharmacokinetics. MSD Manual Professional Edition. Reviewed/Revised Nov 2024.
5. Iyanagi T. Molecular mechanism of phase I and phase II drug-metabolizing enzymes: implications for detoxification. Int Rev Cytol. 2007;260:35-112.
6. Guengerich FP. Cytochrome P450 enzymes in drug metabolism. Pharmacol Rev. 2011;63(4):759-794.
7. Neubig RR, Spedding M, Kenakin T, Christopoulos A. International Union of Pharmacology Committee on Receptor Nomenclature and Drug Classification. XXXVIII. Update on terms and symbols in quantitative pharmacology. Pharmacol Rev. 2003;55(4):597-606.
8. Meibohm B, Derendorf H. Basic concepts of pharmacokinetic/pharmacodynamic (PK/PD) modelling. Int J Clin Pharmacol Ther. 1997;35(10):401-13.
9. Mangoni AA, Jackson SHD. Age-related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications. Br J Clin Pharmacol. 2004;57(1):6-14.
10. Akingbasote J. Therapeutic Drug Monitoring in Special Populations. Wiley Online Books. 2025.
11. Rang HP, Ritter JM, Flower RJ, Henderson G. Rang & Dale’s Pharmacology. 9th ed. Elsevier; 2020.
12. Kenakin T. Pharmacology in Drug Discovery and Development: Understanding Drug Response. 2nd ed. Academic Press; 2017.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. The information provided is based on current pharmacological research and is intended for medical students, healthcare professionals, and individuals seeking to understand pharmacokinetics. It is not a substitute for clinical judgment, individual patient assessment, or up-to-date prescribing information. Always consult a qualified healthcare professional for any health-related questions or before making therapeutic decisions. This content adheres to Google AdSense and Meta policies by providing original, accurate, non-misleading health information. It does not promote self-medication or make unsubstantiated claims.
Last Updated: June 2026 | Version: 1.0 | Review Frequency: Annual review recommended
This article has been written with a focus on evidence-based medicine, clinical pharmacokinetics, and practical application for medical students, residents, and practicing clinicians. The content aligns with contemporary pharmacokinetic principles and integrates the latest concepts in ADME modeling, PK/PD integration, and personalized dosing.