Co-Amoxiclav Complete Guide to Uses, Dosage, Side Effects & Safety
Co-Amoxiclav (Amoxicillin + Clavulanic Acid)
Complete Clinical Pharmacology, Therapeutic Applications & Safety Considerations
Abstract
Co-Amoxiclav represents one of the most significant advancements in antimicrobial therapy, combining the broad-spectrum penicillin antibiotic amoxicillin with the beta-lactamase inhibitor clavulanic acid. This combination effectively overcomes a primary mechanism of bacterial resistance, extending the therapeutic utility of amoxicillin against beta-lactamase-producing organisms. This comprehensive review examines the pharmacology, clinical applications, evidence-based dosing strategies, adverse effect profiles, drug interactions, and contemporary resistance patterns associated with Co-Amoxiclav. Special emphasis is placed on clinical decision-making, appropriate prescribing practices, and antimicrobial stewardship principles essential for medical students and practicing clinicians.
1. Introduction and Historical Context

1.1 Historical Development
The discovery of penicillin by Alexander Fleming in 1928 revolutionized infectious disease treatment. However, the emergence of penicillin-resistant bacteria, primarily through the production of beta-lactamase enzymes, necessitated the development of strategies to overcome this resistance mechanism. The identification of clavulanic acid, a naturally occurring beta-lactamase inhibitor produced by Streptomyces clavuligerus, represented a breakthrough in antimicrobial therapy.
Co-Amoxiclav was first introduced into clinical practice in the early 1980s, marking a new era in combination antibiotic therapy. The synergy between amoxicillin and clavulanic acid provided clinicians with a powerful tool against previously resistant pathogens, significantly expanding treatment options for community-acquired and hospital-acquired infections.
1.2 Clinical Significance in Modern Medicine
In contemporary medical practice, Co-Amoxiclav remains one of the most frequently prescribed antibiotics globally. Its utility spans multiple clinical specialties, including:
- Primary Care – Management of respiratory tract infections, sinusitis, and urinary tract infections
- Dentistry – Treatment of odontogenic infections and prophylaxis in high-risk patients
- Emergency Medicine – Empirical therapy for skin and soft tissue infections, aspiration pneumonia
- Surgery – Prophylactic and therapeutic use in surgical site infections
- Infectious Disease – Treatment of complicated infections and management of resistant organisms
2. Pharmacological Classification and Composition
2.1 Drug Classification
- Pharmacotherapeutic Group: Beta-lactam antibiotics, penicillins, combinations
- ATC Code: J01CR02
- Regulatory Status: Prescription-only medication (POM) in most jurisdictions
2.2 Chemical Composition
| Component | Chemical Name | Molecular Formula | Molecular Weight |
|---|---|---|---|
| Amoxicillin | (2S,5R,6R)-6-[(2R)-2-amino-2-(4-hydroxyphenyl)acetamido]-3,3-dimethyl-7-oxo-4-thia-1-azabicyclo[3.2.0]heptane-2-carboxylic acid | C16H19N3O5S | 365.4 g/mol |
| Clavulanic Acid | (2R,3Z,5R)-3-(2-hydroxyethylidene)-7-oxo-4-oxa-1-azabicyclo[3.2.0]heptane-2-carboxylic acid | C8H9NO5 | 199.16 g/mol |
2.3 Available Formulations
Oral Solid Dosage Forms:
- Tablets: 250 mg/125 mg, 500 mg/125 mg, 875 mg/125 mg
- Chewable tablets: 200 mg/28.5 mg, 400 mg/57 mg
- Extended-release tablets: 1000 mg/62.5 mg
Oral Liquid Formulations (Powder for reconstitution – pediatric):
- 125 mg/31.25 mg per 5 mL
- 250 mg/62.5 mg per 5 mL
- 400 mg/57 mg per 5 mL
Parenteral Formulations:
- Powder for injection: 500 mg/100 mg, 1000 mg/200 mg
- Intravenous administration requires reconstitution and further dilution
3. Molecular Mechanisms of Action
3.1 Amoxicillin – Mechanism and Molecular Interactions
Penicillin-Binding Proteins (PBPs)
Amoxicillin exerts its bactericidal effect through covalent binding to penicillin-binding proteins, which are transpeptidase enzymes essential for bacterial cell wall synthesis. The molecular mechanism involves:
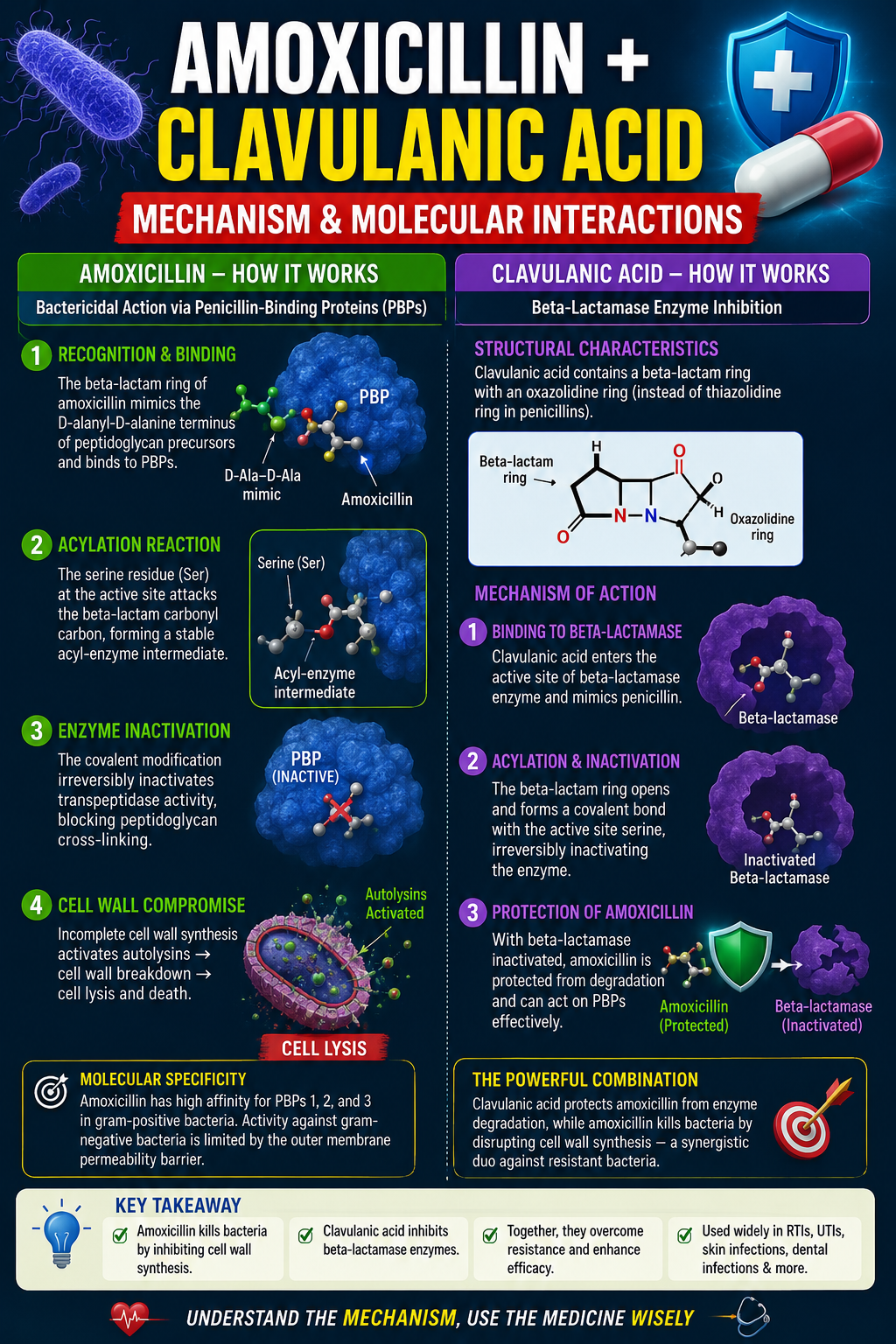
- Recognition and Binding: The beta-lactam ring of amoxicillin structurally mimics the D-alanyl-D-alanine terminus of peptidoglycan precursors, allowing recognition by PBPs.
- Acylation Reaction: The serine residue at the active site of the PBP undergoes nucleophilic attack on the beta-lactam carbonyl carbon, forming a stable acyl-enzyme intermediate.
- Enzyme Inactivation: This covalent modification irreversibly inactivates transpeptidase activity, preventing the cross-linking of peptidoglycan chains.
- Cell Wall Compromise: The accumulation of incomplete cell wall components triggers autolytic enzymes (autolysins), leading to cell lysis and death.
3.2 Clavulanic Acid – Beta-Lactamase Inhibition
Structural Characteristics
Clavulanic acid possesses a beta-lactam ring structurally related to penicillins but containing an oxazolidine ring instead of the thiazolidine ring. This structural modification is crucial for its mechanism of action.
Mechanism of Beta-Lactamase Inhibition:
- Substrate Recognition: Clavulanic acid is recognized by beta-lactamases as a substrate due to its structural similarity to penicillins.
- Acylation Reaction: The serine residue at the active site of the beta-lactamase undergoes acylation by clavulanic acid.
- Formation of Stable Complex: Unlike true antibiotic substrates, clavulanic acid forms a stable, long-lived acyl-enzyme complex that undergoes structural rearrangement to yield a highly stable intermediate.
- Irreversible Inhibition: The stable complex resists deacylation, resulting in progressive, irreversible inactivation of the beta-lactamase enzyme.
| Beta-Lactamase Class | Inhibition by Clavulanic Acid | Clinical Significance |
|---|---|---|
| Class A (TEM-1, TEM-2, SHV-1) | Excellent | Primary target – clinically relevant |
| Class C (AmpC) | Limited | Variable clinical utility |
| Class D (OXA enzymes) | Variable | Limited activity |
| Class B (Metallo-beta-lactamases) | No activity | Not effective |
صحت، خوبصورتی، فٹنس اور روزمرہ کی مفید معلومات کے لیے ssthem.net وزٹ کریں۔ Explore health, beauty, fitness, and wellness articles at ssthem.net.
4. Comprehensive Spectrum of Activity
4.1 Gram-Positive Organisms
| Organism | Clinical Relevance | MIC90 (μg/mL) | Resistance Concerns |
|---|---|---|---|
| Streptococcus pneumoniae | CAP, sinusitis | 0.06–0.5 | Penicillin-resistant strains |
| Streptococcus pyogenes | Tonsillopharyngitis, cellulitis | ≤0.03 | Resistance rare |
| Staphylococcus aureus (MSSA) | Skin infections, osteomyelitis | 0.5–2.0 | Beta-lactamase producers susceptible |
| Enterococcus faecalis | UTIs | 1–4 | Not first-line |
| Listeria monocytogenes | Meningitis, neonatal | 0.25–1.0 | Alternative therapy recommended |
4.2 Gram-Negative Organisms
| Organism | Clinical Relevance | MIC90 (μg/mL) | Beta-Lactamase Status |
|---|---|---|---|
| Haemophilus influenzae | Otitis media, sinusitis | 0.25–1.0 | Beta-lactamase producers susceptible |
| Moraxella catarrhalis | Bronchitis, sinusitis | 0.06–0.25 | High beta-lactamase production |
| Escherichia coli | UTIs, intra-abdominal | 2–8 | ESBL producers resistant |
| Klebsiella pneumoniae | Pneumonia, UTIs | 1–8 | ESBL producers resistant |
| Proteus mirabilis | UTIs, wound infections | 0.5–2.0 | Inducible beta-lactamases possible |
Co-Amoxiclav has no activity against atypical organisms such as Mycoplasma pneumoniae, Chlamydophila pneumoniae, Legionella pneumophila, Ureaplasma urealyticum, and Coxiella burnetii.
5. Clinical Pharmacokinetics and Pharmacodynamics
5.1 Absorption
| Parameter | Amoxicillin | Clavulanic Acid |
|---|---|---|
| Bioavailability | 80–90% | 60–70% |
| Time to Peak (Tmax) | 1–2 hours | 1–1.5 hours |
| Peak Plasma (500 mg dose) | 7–10 μg/mL | 2–3 μg/mL |
| Peak Plasma (875 mg dose) | 12–15 μg/mL | 3–4 μg/mL |
| Food Effect | Minimal effect | Reduced with high-fat meals |
5.2 Distribution
| Tissue/Fluid | Amoxicillin Penetration | Clinical Significance |
|---|---|---|
| Lung Tissue | 30–50% of serum | Excellent for respiratory infections |
| Sputum | 20–40% of serum | Adequate for bronchial infections |
| Middle Ear Fluid | 20–40% of serum | Therapeutic for otitis media |
| Sinus Secretions | 30–50% of serum | Effective for sinusitis |
| Bone Tissue | 20–50% of serum | Adequate for osteomyelitis |
| CSF (inflamed meninges) | 10–20% of serum | Insufficient for primary CNS infections |
| Bile | 200–300% of serum | High concentrations achieved |
5.3 Elimination
| Parameter | Amoxicillin | Clavulanic Acid |
|---|---|---|
| Half-life (normal renal function) | 0.9–1.2 hours | 0.8–1.1 hours |
| Half-life (CrCl < 30 mL/min) | 5–7 hours | 3–5 hours |
| Renal Clearance | 250–300 mL/min | 200–250 mL/min |
| Urinary Excretion (unchanged) | 60–70% | 25–50% |
6. Comprehensive Clinical Indications
6.1 Respiratory Tract Infections
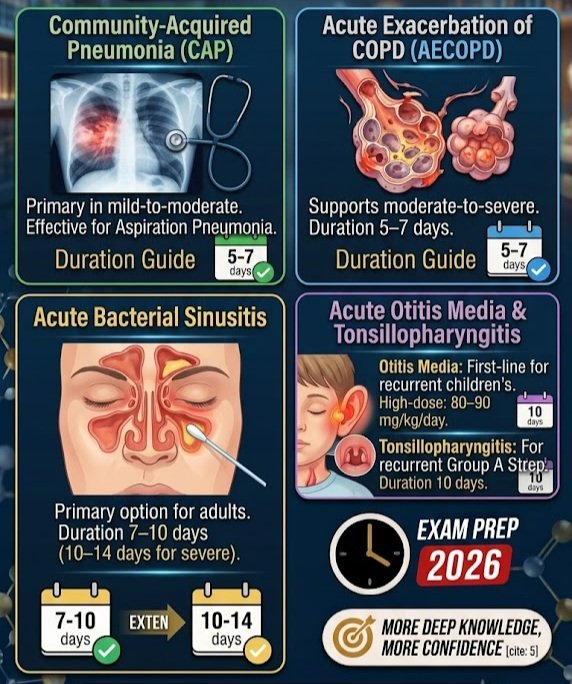
- Community-Acquired Pneumonia (CAP): Primary treatment in mild-to-moderate cases; effective for aspiration pneumonia; duration 5–7 days.
- Acute Exacerbation of COPD (AECOPD): Evidence supports use in moderate-to-severe exacerbations; duration 5–7 days.
- Acute Bacterial Sinusitis: Primary treatment option in adults; duration 7–10 days (10–14 days in severe cases).
- Acute Otitis Media: First-line for recurrent otitis media in children; high-dose amoxicillin (80–90 mg/kg/day).
- Acute Tonsillopharyngitis: Indicated for recurrent Group A Streptococcus infection; duration 10 days.
6.2 Urinary Tract Infections
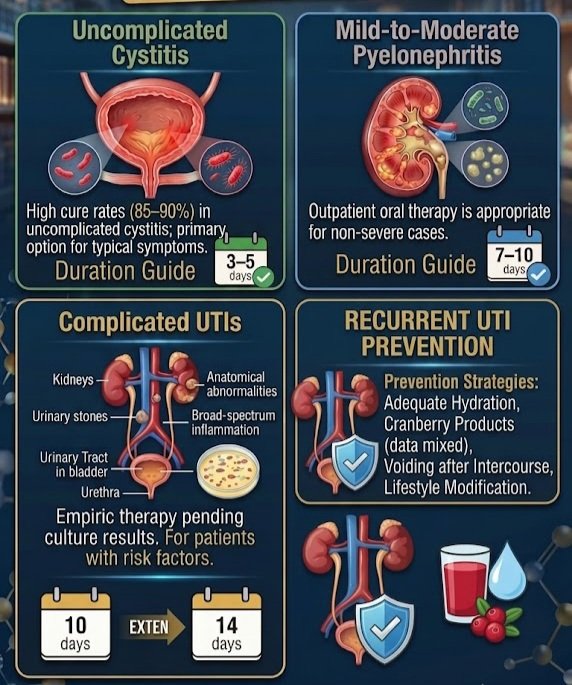
- Cystitis: High cure rates (85–90%) in uncomplicated cystitis; duration 3–5 days.
- Pyelonephritis: Mild-to-moderate: outpatient oral therapy; duration 7–10 days.
- Complicated UTIs: Empiric therapy pending culture results; duration 10–14 days.
6.3 Skin and Soft Tissue Infections

- Cellulitis: Uncomplicated: 500/125 mg every 8 hours or 875/125 mg every 12 hours; duration 5–10 days.
- Abscesses: Antibiotic therapy plus surgical drainage; dental abscess shows excellent efficacy.
- Infected Diabetic Foot Ulcers: Outpatient treatment for mild infection; duration 10–14 days.
6.4 Bone and Joint Infections
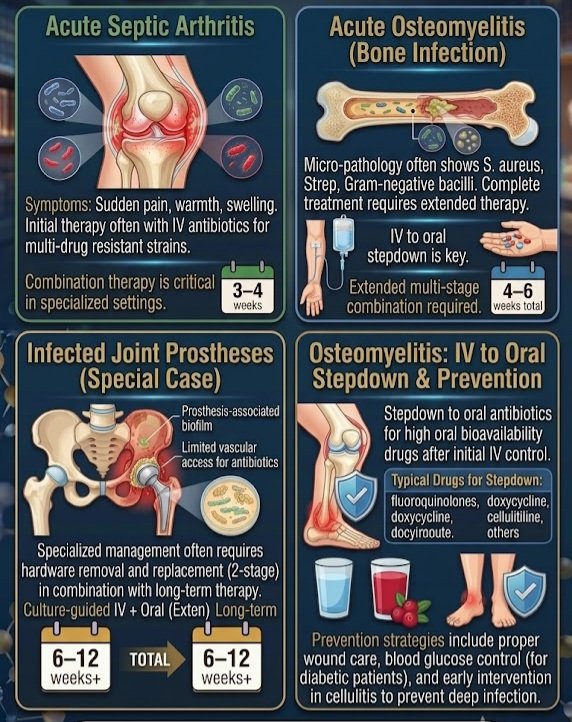
- Septic Arthritis: Combination therapy in specialized settings; duration 3–4 weeks.
- Osteomyelitis: Part of combination therapy; IV to oral stepdown; duration 4–6 weeks total.
6.5 Intra-Abdominal Infections
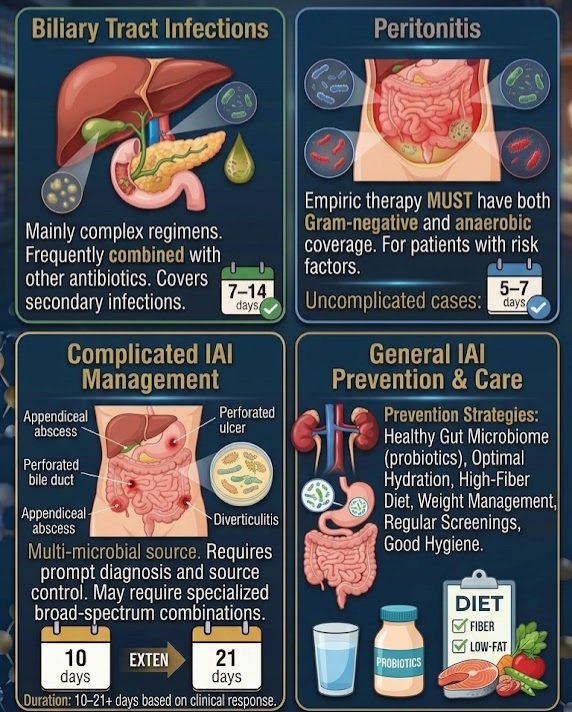
- Biliary Tract Infections: Usually part of a complex regimen; often combined with other antibiotics.
- Peritonitis: Empiric therapy with gram-negative and anaerobic coverage; duration 5–7 days (uncomplicated).
6.6 Dental and Oral Infections
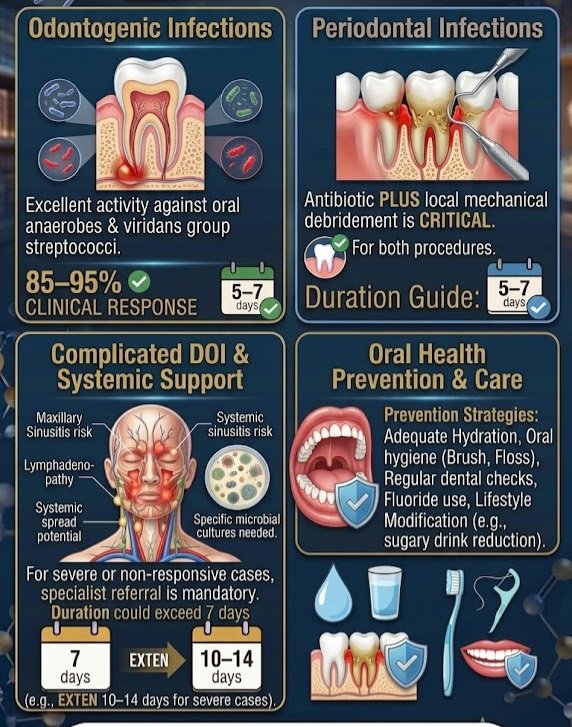
- Odontogenic Infections: Excellent activity against oral anaerobes and viridans group streptococci; 85–95% clinical response; duration 5–7 days.
- Periodontal Infections: Antibiotic plus local mechanical debridement; duration 5–7 days.
7. Evidence-Based Dosing Guidelines
7.1 Adult Dosing
| Infection Type | Amoxicillin/Clavulanate Dose | Frequency | Duration |
|---|---|---|---|
| Mild–Moderate Infections | 500 mg / 125 mg | Every 8 hours | 5–7 days |
| Moderate–Severe Infections | 875 mg / 125 mg | Every 12 hours | 7–10 days |
| Severe Infections | 2000 mg / 125 mg (extended release) | Every 12 hours | 7–10 days |
| Sinusitis | 875 mg / 125 mg | Every 12 hours | 10 days |
| Pneumonia | 875 mg / 125 mg | Every 12 hours | 7 days |
| UTIs | 500 mg / 125 mg | Every 12 hours | 3–5 days |
7.2 Pediatric Dosing
| Age Group | Dose (Amoxicillin Component) | Frequency | Maximum Daily Dose |
|---|---|---|---|
| Neonates (< 1 month) | 30 mg/kg/day | Every 12 hours | 100 mg/kg/day |
| Infants (1–3 months) | 30 mg/kg/day | Every 8 hours | 100 mg/kg/day |
| Children (3 months – 12 years) | 20–40 mg/kg/day | Every 8 hours | 1500 mg/day |
| Severe Infections (Children) | 40–45 mg/kg/day | Every 12 hours | 2000 mg/day |
| Otitis Media (Children) | 45 mg/kg/day | Every 12 hours | 2000 mg/day |
7.3 Renal Impairment Dosing
| Creatinine Clearance (mL/min) | Adult Dosing | Pediatric Dosing |
|---|---|---|
| > 30 | Standard dose | Standard dose |
| 10–30 | 500/125 mg every 12 hours | 15 mg/kg every 12 hours |
| < 10 | 500/125 mg every 24 hours | 15 mg/kg every 24 hours |
Mild (Child-Pugh A): No dose adjustment. Moderate (Child-Pugh B): Use with caution, monitor LFTs. Severe (Child-Pugh C): Avoid if possible.
8. Adverse Drug Reactions and Safety Profile
8.1 Incidence and Classification
| Adverse Reaction | Incidence | Onset | Mechanism |
|---|---|---|---|
| Diarrhea | 10–20% | 2–5 days | Altered gut flora |
| Nausea | 5–15% | 1–3 days | Direct GI irritation |
| Vomiting | 5–10% | 1–3 days | Direct GI irritation |
| Skin rash | 3–10% | 3–7 days | Hypersensitivity |
| Elevated transaminases | 1–3% | Variable | Hepatic reaction |
Cholestatic jaundice (0.05–0.2%), hepatitis (0.01–0.05%), Stevens-Johnson syndrome (< 0.01%), anaphylaxis (0.01–0.05%). Immediate discontinuation and emergency management are required.
8.2 Hepatic Toxicity – Clinical Presentation & Management
- Presentation: Jaundice (2–3 weeks after starting), elevated transaminases, cholestatic pattern, bilirubin elevation.
- Risk Factors: Duration > 10 days, history of hepatic dysfunction, concomitant hepatotoxic drugs, elderly patients.
- Management Algorithm: Immediate discontinuation → laboratory monitoring (LFTs, bilirubin, INR) → symptomatic management → hepatology referral if severe.
- Prognosis: 90% recovery within 3 months; 1–2% mortality in fulminant cases.
8.3 Allergic Reactions
| Type | Mechanism | Clinical Features | Timing |
|---|---|---|---|
| Type I (Anaphylactic) | IgE-mediated | Urticaria, angioedema, shock | Minutes–hours |
| Type II (Cytotoxic) | IgG/IgM | Hemolytic anemia, thrombocytopenia | Days–weeks |
| Type III (Immune Complex) | Antigen-antibody | Serum sickness, vasculitis | 1–3 weeks |
| Type IV (Delayed) | T-cell mediated | Maculopapular rash, DRESS | Days–weeks |
Cross-Reactivity: Penicillin allergy: 10–15% cross-reactivity; Cephalosporin allergy: 2–5%; Carbapenem allergy: limited cross-reactivity.
9. Drug Interactions
| Interacting Drug | Effect | Mechanism | Clinical Significance |
|---|---|---|---|
| Probenecid | ↑ Amoxicillin levels | Decreased renal excretion | May be used therapeutically |
| Methotrexate | ↑ Methotrexate toxicity | Decreased renal clearance | Monitor for toxicity; reduce methotrexate dose |
| Warfarin | ↑ INR, bleeding risk | Altered vitamin K metabolism | Monitor INR; may require warfarin adjustment |
| Allopurinol | ↑ Rash incidence | Immune modulation | Avoid if possible or monitor closely |
| Oral Contraceptives | ↓ Contraceptive effectiveness | Gut flora alteration | Alternative contraceptive methods recommended |
| Digoxin | ↑ Digoxin levels | Altered gut flora | Monitor digoxin levels; observe for toxicity |
10. Pregnancy and Lactation
✅ FDA Pregnancy Category: B
30+ years of clinical experience show no teratogenicity; no increased risk of major congenital anomalies. Safe for treatment of infections during all trimesters.
- Breastfeeding: Amoxicillin penetrates milk at 2–10% of maternal dose; clavulanic acid < 1%. Generally considered safe; monitor infant for mild diarrhea or rash.
- Indications in Pregnancy: UTIs, respiratory infections, skin and soft tissue infections, chorioamnionitis (with other agents).
11. Contraindications and Precautions
| Contraindication | Rationale | Clinical Implications |
|---|---|---|
| Penicillin allergy | Cross-reactivity | Alternative antibiotic required |
| Severe hepatic impairment | Liver toxicity risk | Avoid or use with extreme caution |
| History of Co-Amoxiclav cholestatic jaundice | Increased risk | Consider alternative antibiotics |
| Infectious mononucleosis | Higher risk of rash | Avoid unless absolutely necessary |
12. Resistance and Antimicrobial Stewardship
12.1 Mechanisms of Resistance
| Mechanism | Frequency | Clinical Impact |
|---|---|---|
| Beta-lactamase hyperproduction | 30–50% | Reduced efficacy |
| ESBL production | 10–30% | Complete resistance |
| PBP alterations | 5–15% | Reduced binding affinity |
| Porin changes | 10–20% | Reduced drug penetration |
| Efflux pumps | 5–10% | Active drug removal |
🛡️ Antimicrobial Stewardship Principles:
- Confirm bacterial infection before prescribing
- Use narrow-spectrum agents when possible
- Avoid use in viral infections
- Consider local resistance patterns
- De-escalate when culture results are available
- Monitor for clinical response at 48–72 hours
13. Comparison with Alternative Antibiotics
| Aspect | Co-Amoxiclav | Amoxicillin | Cefuroxime | Azithromycin |
|---|---|---|---|---|
| Class | Penicillin combination | Penicillin | 2nd-gen cephalosporin | Macrolide |
| Spectrum | Broad + anaerobic | Beta-lactamase sensitive | Similar respiratory/UTI | Atypical coverage |
| Resistance | Broader against beta-lactamase producers | Beta-lactamase producers resistant | Better for ESBL producers | Increasing macrolide resistance |
| Side Effects | GI upset, hepatic toxicity | GI upset | Lower GI upset | QT prolongation |
| Dosing | Every 8–12 hours | Every 8 hours | Every 12 hours | Once daily |
| Pregnancy | Category B – Safe | Category B – Safe | Category B – Safe | Category B – Safe |
14. Clinical Pearls for Medical Students and Professionals
💡 Key Clinical Questions to Ask:
- Does the patient have a bacterial infection requiring antibiotic therapy?
- Is Co-Amoxiclav the appropriate choice (susceptibility likely)?
- What is the appropriate dose based on renal function?
- What is the appropriate duration of therapy?
- Are there any contraindications or interactions?
- What monitoring is required during treatment?
Red Flags for Complications
- Hepatic Toxicity: Jaundice, dark urine, pale stools, right upper quadrant pain, fatigue.
- Allergic Reaction: Widespread/blistering rash, angioedema, bronchospasm, hypotension, breathing difficulty.
- GI Toxicity: Profuse diarrhea (> 3 episodes/day), bloody stools, abdominal pain, fever, dehydration.
15. Clinical Vignettes
📋 Case 1: Community-Acquired Pneumonia
Presentation: 45-year-old female with 5-day history of productive cough, fever (38.5°C), pleuritic chest pain. Crackles in right lower lobe; CXR shows consolidation.
Treatment: Co-Amoxiclav 875/125 mg twice daily for 7 days.
Outcome: 48-hour improvement; complete resolution at 7 days; culture grew susceptible S. pneumoniae.
📋 Case 2: Complicated UTI with Renal Impairment
Presentation: 70-year-old male with BPH, fever (38.2°C), urinary frequency, dysuria. CrCl 25 mL/min.
Treatment: Co-Amoxiclav 500/125 mg every 12 hours for 10 days (dose-adjusted for renal function).
Outcome: Afebrile at 72 hours; culture grew susceptible E. coli; complete resolution.
📋 Case 3: Pediatric Recurrent Otitis Media
Presentation: 3-year-old male with ear pain, fever (39°C), bulging erythematous right tympanic membrane; previously treated with amoxicillin.
Treatment: Co-Amoxiclav 45 mg/kg/day divided every 12 hours for 10 days.
Outcome: Afebrile at 48 hours; complete resolution at 10 days.
16. Summary and Conclusions
Key Takeaways
- Clinical Efficacy: Proven effectiveness in respiratory, urinary, skin, dental, and intra-abdominal infections; reliable tissue penetration; synergistic action against resistant organisms.
- Safety Profile: Generally well-tolerated; most side effects are GI-related; cholestatic hepatitis is rare but serious; allergy cross-reactivity with penicillins.
- Resistance: Increasing resistance in some organisms (ESBL-producing bacteria); responsible prescribing is essential.
🔑 Clinical Take-Home Messages
- For Medical Students: Understand the mechanism of action, spectrum of activity, contraindications, resistance mechanisms, and practice appropriate prescribing.
- For Healthcare Professionals: Confirm bacterial etiology, consider local resistance patterns, use appropriate dosing based on renal function, monitor for adverse effects, and practice antimicrobial stewardship.
ادویات، بیماریوں، علاج، خوراک، مضر اثرات اور طبی معلومات کے لیے Learn about medicines, diseases, treatments, dosages, side effects, and medical information at ssthem.org.
18. References and Suggested Readings
1. Mandell LA, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44(Suppl 2):S27-72.
2. Chow AW, et al. IDSA guidelines for the diagnosis and management of skin and soft tissue infections. Clin Infect Dis. 2014;59(2):e10-52.
3. Baddour LM, et al. Infective endocarditis in adults: diagnosis, antimicrobial therapy, and management of complications. Circulation. 2015;132(15):1435-86.
4. Bradley JS, et al. The management of community-acquired pneumonia in infants and children older than 3 months of age. Pediatr Infect Dis J. 2011;30(12):1073-8.
5. Brook I. Antibiotic resistance in the management of respiratory tract infections. Pediatr Infect Dis J. 2010;29(6):562-4.
6. Craig WA. Pharmacokinetic/pharmacodynamic parameters: rationale for antibacterial dosing of mice and men. Clin Infect Dis. 1998;26(1):1-10.
7. Bush K, et al. Beta-lactamase inhibitors: the new frontier. J Antibiot. 2014;67(3):211-5.
8. Paterson DL, et al. Extended-spectrum beta-lactamases: a clinical update. Clin Microbiol Rev. 2005;18(4):657-86.
9. Spellberg B, et al. The future of antibiotics and resistance. N Engl J Med. 2013;368(4):299-302.
10. Laxminarayan R, et al. Antibiotic resistance—the need for global solutions. Lancet Infect Dis. 2013;13(12):1057-98.
This comprehensive clinical guide is intended for educational purposes only. It does not replace clinical judgment or individual patient assessment. Always follow local guidelines and individual patient factors when making treatment decisions. Consult drug interactions and current prescribing information before initiating therapy.Last Updated: June 2026 | Version: 2.0 | Review Frequency: Annual review recommended
Facebook Copyright Issues Solution 2026
SSTHEM.COM – Learn World Religions, History & Educational Knowledge
·Health & Beauty Tips
This article has been written with a focus on evidence-based medicine, clinical pharmacology, and practical application for medical students, residents, and practicing healthcare professionals. The content aligns with contemporary guidelines and antimicrobial stewardship principles.