Best Medicine for Tooth Pain Evidence‑Based Guide for BDS
What Is the Best Medicine for Tooth Pain?
A Complete Evidence-Based Guide for BDS Students & Dental Professionals
Toothache is one of the most common presentations in dental and emergency settings, with someone visiting a hospital emergency department for a dental condition approximately every 15 seconds in the United States. This comprehensive evidence-based guide examines the pharmacological management of dental pain, addressing the clinical question: “What is the best medicine for tooth pain?” The answer depends on the underlying etiology, pain intensity, patient medical history, and contraindications. Drawing on current clinical practice guidelines from the American Dental Association, systematic reviews, and meta-analyses, this article provides BDS students with a thorough understanding of analgesic pharmacology, evidence-based prescribing, and antimicrobial stewardship principles essential for safe and effective clinical practice.
1. Introduction
Dental pain is one of the most prevalent and distressing conditions encountered in clinical practice. Approximately 70% of emergency dental visits occur outside regular business hours, placing emergency physicians and dental professionals in a position to mitigate dental pain until definitive care can be obtained. For BDS students, understanding the pharmacology of dental pain management is not merely an academic exercise—it is a clinical imperative that directly impacts patient outcomes, safety, and quality of life.
The question “What is the best medicine for tooth pain?” is deceptively simple. The answer depends on multiple factors: the underlying etiology of the pain, the patient’s medical history, the presence of contraindications, the intensity of pain, and the clinical setting. This article provides a comprehensive, evidence-based guide to the pharmacological management of dental pain, drawing on current clinical practice guidelines, systematic reviews, and meta-analyses. It is designed specifically for BDS students who require a deep understanding of analgesic pharmacology to make informed clinical decisions.
1.1 The Clinical Burden of Dental Pain
Dental pain significantly impacts quality of life, sleep, work productivity, and overall well-being. In the United States alone, over 2 million emergency department visits annually are attributed to dental conditions, with an estimated cost exceeding $1.6 billion per year. The most common causes include dental caries (31%), pulpitis (22%), and pericoronitis (12%). The prevalence of dental pain underscores the critical need for healthcare professionals—particularly dental students and practitioners—to master evidence-based pain management strategies.
Key Insight: The American Dental Association (ADA) and multiple systematic reviews have concluded that NSAIDs—particularly ibuprofen—are more effective than opioid-containing medications for acute dental pain in many patients. The combination of ibuprofen and paracetamol provides superior analgesia compared with either drug alone and performs as well as or better than opioids with fewer adverse effects.
2. Physiology of Dental Pain
 Dental pain falls under the broader category of orofacial pain and is processed by the trigeminal nervous system. The trigeminal nerve (cranial nerve V) is responsible for detecting sensations in the face, including nociception from the teeth and surrounding oral structures.
Dental pain falls under the broader category of orofacial pain and is processed by the trigeminal nervous system. The trigeminal nerve (cranial nerve V) is responsible for detecting sensations in the face, including nociception from the teeth and surrounding oral structures.
2.1 The Dentin-Pulp Complex
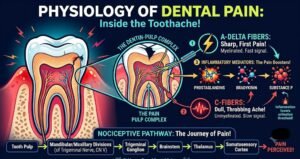
The dentin-pulp complex is central to the unique biology of dental pain. Dental afferent nerve fibers, whose cell bodies reside within the trigeminal ganglion, enter the tooth via the apical foramina. These fibers include both myelinated A-delta fibers and unmyelinated C-fibers.
- A-delta fibers – Responsible for sharp, well-localized pain; mediate the initial rapid response to stimuli
- C-fibers – Mediate dull, aching, and poorly localized pain; responsible for the chronic, throbbing nature of pulpitis
2.2 Nociceptive Pathways
Signals from the dental pulp travel via the mandibular and maxillary divisions of the trigeminal nerve to the brainstem, where they synapse with second-order neurons in the trigeminal nuclei. From there, the signal ascends to higher brain centers, including the thalamus and somatosensory cortex, where pain is perceived.
2.3 Inflammatory Mediators
Inflammation is a key mechanism behind most types of dental pain. When dental pulp is irritated by caries, trauma, or bacterial invasion, inflammatory mediators such as prostaglandins, bradykinin, substance P, and cytokines are released. These mediators sensitize nociceptors, lowering their threshold for activation and amplifying pain signals. This is why anti-inflammatory drugs—particularly NSAIDs—are so effective in managing dental pain.
3. Causes of Tooth Pain
 Toothache is usually caused by dental caries and its consequences. Caries causes pain when the lesion extends through the enamel into dentin, resulting in sufficient demineralization to cause cavitation.
Toothache is usually caused by dental caries and its consequences. Caries causes pain when the lesion extends through the enamel into dentin, resulting in sufficient demineralization to cause cavitation.
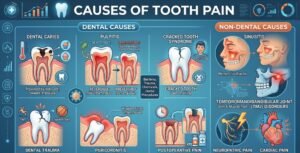
3.1 Dental Causes
- Dental caries – The most common cause. Pain is typically provoked by thermal stimuli (hot or cold), sweet foods, or occlusal pressure.
- Pulpitis – Inflammation of the pulp tissue due to bacteria, trauma, chemicals, or dental procedures. Reversible pulpitis is characterized by short-lived pain to stimuli; irreversible pulpitis involves spontaneous, paroxysmal episodes that may worsen at night.
- Cracked tooth syndrome – Incomplete fractures of the tooth that cause pain on biting.
- Dental trauma – Falls, blows to the face, or sports injuries.
- Pericoronitis – Inflammation around a partially erupted wisdom tooth.
- Postoperative pain – Following extractions, root canal treatment, or other dental procedures.
- Dental abscess – Localized collection of pus due to bacterial infection.
3.2 Non-Dental Causes
- Sinusitis – Maxillary sinus inflammation can mimic toothache in the upper posterior teeth.
- Temporomandibular joint disorders – Pain in the jaw joint and muscles of mastication.
- Neuropathic pain – Such as trigeminal neuralgia or atypical odontalgia.
- Cardiac pain – Rarely, myocardial ischemia can present as jaw or tooth pain.
4. Classification of Dental Pain
 Dental pain can be classified according to its origin and characteristics:
Dental pain can be classified according to its origin and characteristics:
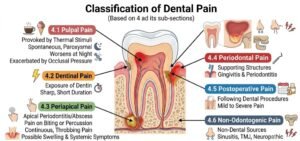
4.1 Pulpal Pain
Originating from the dental pulp, this pain is typically:
- Provoked by thermal stimuli (hot or cold)
- Spontaneous and paroxysmal in irreversible pulpitis
- Worsens at night
- Exacerbated by occlusal pressure
4.2 Dentinal Pain
Caused by exposure of dentin due to cavities, tooth wear, or abrasive substances. Pain is usually sharp and of short duration.
4.3 Periapical Pain
Pain from the tissues surrounding the root apex, often due to apical periodontitis or abscess. Characterized by:
- Pain on biting or percussion
- Continuous, throbbing pain
- Possible swelling and systemic symptoms
4.4 Periodontal Pain
Pain from the supporting structures of the tooth, including gingivitis and periodontitis.
4.5 Postoperative Pain
Pain following dental procedures, ranging from mild discomfort to severe pain after surgical extractions.
4.6 Non-Odontogenic Pain
Pain arising from non-dental sources, including sinusitis, TMJ disorders, and neuropathic conditions.
5. The Pain Pathway
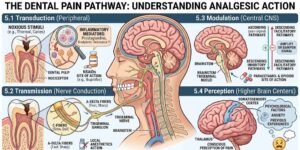 Understanding the pain pathway is essential for appreciating how different analgesics work. The dental pain pathway can be summarized in four stages:
Understanding the pain pathway is essential for appreciating how different analgesics work. The dental pain pathway can be summarized in four stages:
5.1 Transduction
Noxious stimuli (thermal, mechanical, or chemical) activate nociceptors in the dental pulp. Inflammatory mediators such as prostaglandins, bradykinin, and substance P sensitize these nociceptors, lowering their activation threshold.
5.2 Transmission
The pain signal travels along A-delta and C-fibers from the pulp to the trigeminal ganglion, then via the trigeminal nerve to the brainstem trigeminal nuclei.
5.3 Modulation
In the brainstem, the signal is modulated by descending inhibitory pathways that can either amplify or dampen the pain signal. This is where centrally acting drugs like paracetamol exert some of their effects.
5.4 Perception
The processed signal reaches the thalamus and cerebral cortex, where pain is consciously perceived. Psychological factors, anxiety, and previous experiences can influence pain perception.
6. How Painkillers Work: Mechanisms of Action
6.1 NSAIDs (Peripheral Action)
NSAIDs act peripherally, meaning they help with pain by reducing inflammation at the site where it is occurring. They work by inhibiting cyclo-oxygenase (COX) enzymes (COX-1 and COX-2), which are involved in prostaglandin synthesis via the arachidonic acid pathway.
- COX-1 is constitutively expressed and protects the gastric mucosa, maintains renal blood flow, and supports platelet aggregation.
- COX-2 is induced by inflammation and produces prostaglandins that mediate pain, fever, and inflammation.
By reducing prostaglandin synthesis, NSAIDs decrease inflammation, lower peripheral nociceptor sensitization, and thereby reduce pain.
6.2 Acetaminophen (Central Action)
Acetaminophen (paracetamol) acts primarily within the central nervous system. While the precise mechanism is not fully understood, it is believed to inhibit the peroxidase portion of cyclooxygenase (prostaglandin H synthase). It raises the pain threshold in the central nervous system and reduces fever. Unlike NSAIDs, it has minimal anti-inflammatory effect.
6.3 Opioids (Central Action)
Opioids bind to mu, kappa, and delta opioid receptors in the central nervous system and peripheral tissues. They inhibit the release of neurotransmitters involved in pain transmission (such as substance P) and activate descending inhibitory pathways.
6.4 Local Anesthetics
Local anesthetics block voltage-gated sodium channels on nerve membranes, preventing the generation and conduction of action potentials. This produces reversible loss of sensation in the targeted area.
7. Evidence-Based Clinical Guidelines
Several major organizations have published evidence-based guidelines for managing acute dental pain. The following recommendations represent the current consensus:
7.1 American Dental Association (ADA) Guidelines
The ADA, in collaboration with the University of Pittsburgh School of Dental Medicine and the University of Pennsylvania School of Dental Medicine, has developed clinical practice guidelines for managing acute dental pain. Key recommendations include:
- First-line therapy: NSAIDs alone (e.g., 400 mg ibuprofen or 440 mg naproxen sodium) OR in combination with acetaminophen (e.g., 500–1000 mg).
- When NSAIDs are contraindicated: Acetaminophen alone at full therapeutic dose (e.g., 1,000 mg).
- Inadequate pain control: If NSAIDs alone prove inadequate, the guideline suggests adding acetaminophen. If pain persists despite combination therapy, a low-dose opioid may be considered for a maximum of three days.
- Avoid “just in case” opioids: Clinicians should avoid prescribing opioids prophylactically.
7.2 Evidence from 87 RCTs
Evidence from 87 randomized controlled trials indicates that NSAIDs—alone or combined with acetaminophen—are more effective for postoperative dental pain relief than opioids.
7.3 American Journal of Emergency Medicine Guidelines
A 2024 guideline published in the American Journal of Emergency Medicine concluded that:
- NSAIDs alone or in combination with acetaminophen are the first-line therapy for managing acute dental pain following tooth extraction(s) and temporary management of toothache.
- Opioids should be reserved for clinical situations when first-line therapy is insufficient or contraindications to NSAIDs exist.
- Opioids should only be used when NSAIDs are ineffective or contraindicated.
7.4 CDC and FDA Alignment
Both guidelines are endorsed by the ADA and expand recommendations from the Centers for Disease Control and Prevention and the FDA Report on Evidence-based Opioid Analgesic Prescribing Guidelines.
7.5 Summary of Recommendations
| Clinical Situation | Recommended Therapy |
|---|---|
| Mild to moderate inflammatory dental pain | NSAID alone (ibuprofen 400 mg or naproxen 440 mg) |
| Moderate to severe dental pain | NSAID + acetaminophen (e.g., ibuprofen 400 mg + paracetamol 500–1000 mg) |
| NSAID contraindicated | Acetaminophen 1000 mg |
| Inadequate response to combination | Consider low-dose opioid for ≤3 days |
| Immediate relief needed | Local anesthetic (e.g., 2% lidocaine with epinephrine) |
8. Non-Steroidal Anti-Inflammatory Drugs (NSAIDs)
NSAIDs are the cornerstone of acute dental pain management. Their anti-inflammatory properties directly address the underlying pathophysiology of most toothaches.
8.1 Ibuprofen
Ibuprofen is a non-selective COX inhibitor that is widely considered the first-line analgesic for inflammatory dental pain.
- Mechanism: Inhibits COX-1 and COX-2 enzymes, reducing prostaglandin synthesis.
- Onset: Approximately 30 minutes.
- Duration: 4–6 hours.
- Typical dose (adult): 200–400 mg every 6–8 hours; maximum 1,200–2,400 mg/day.
- Clinical use: First-line for most dental pain, including pulpitis, postoperative pain, and pericoronitis.
- Evidence: Systematic reviews consistently support ibuprofen as effective for postoperative dental pain.
8.2 Naproxen
Naproxen is a non-selective NSAID with a longer duration of action than ibuprofen.
- Mechanism: Similar to ibuprofen—COX-1 and COX-2 inhibition.
- Onset: 1–2 hours.
- Duration: 8–12 hours.
- Typical dose (adult): 220–440 mg twice daily; maximum 1,375–1,500 mg/day.
- Clinical use: When longer-acting analgesia is desired. The ADA recommends naproxen sodium 440 mg as an alternative to ibuprofen 400 mg.
- Advantage: Less frequent dosing improves patient compliance.
8.3 Diclofenac
Diclofenac is a potent NSAID with strong anti-inflammatory activity.
- Mechanism: Potent COX-1 and COX-2 inhibition.
- Onset: 30–60 minutes.
- Duration: 6–8 hours.
- Typical dose (adult): 50 mg three times daily.
- Clinical use: Useful after oral surgery and for more severe inflammatory pain.
- Evidence: Diclofenac + acetaminophen provided the greatest pain reduction at 6–8 hours in a recent meta-analysis (MD: -6.28, 95% CI: -11.99 to -0.56).
8.4 Ketorolac
Ketorolac is a high-potency NSAID frequently used for short-term postoperative dental pain.
- Mechanism: Potent COX-1 and COX-2 inhibition.
- Onset: 30–60 minutes.
- Duration: 4–6 hours.
- Typical dose (adult): 10–20 mg every 4–6 hours; maximum 40 mg/day.
- Clinical use: Short-term (≤5 days) management of moderate to severe postoperative pain.
- Evidence: Ketorolac 10 mg and 20 mg were both more efficacious than ketoprofen 50 mg. In pediatric patients, ketorolac was significantly more effective than acetaminophen at 2 hours postoperatively.
- Caution: Limited duration of use because of gastrointestinal and renal risks.
8.5 Celecoxib
Celecoxib is a selective COX-2 inhibitor.
- Mechanism: Selective COX-2 inhibition; spares COX-1, potentially reducing gastrointestinal side effects.
- Typical dose (adult): 100–200 mg once or twice daily; maximum 400 mg/day.
- Clinical use: Selected patients at risk of gastrointestinal bleeding or those intolerant to non-selective NSAIDs.
- Note: The use of celecoxib for management of acute dental pain is considered “off-label” in some jurisdictions.
- Evidence: Celecoxib 200 mg demonstrated a risk ratio of 15.86 for pain relief in dental pain compared with placebo (95% CI: 5.14–48.99).
All NSAIDs carry risks of gastrointestinal bleeding, renal impairment, and cardiovascular events. Use the lowest effective dose for the shortest duration. Assess patient risk factors before prescribing.
9. Acetaminophen (Paracetamol)
Acetaminophen is a centrally acting analgesic and antipyretic drug.
- Mechanism: Inhibits the peroxidase portion of cyclooxygenase (prostaglandin H synthase) in the central nervous system. It raises the pain threshold and reduces fever.
- Onset: 30–60 minutes.
- Duration: 4–6 hours.
- Typical dose (adult): 500–1,000 mg every 4–6 hours; maximum 3,000–4,000 mg/day.
- Clinical use:
- Mild to moderate dental pain
- When NSAIDs are contraindicated
- In combination with NSAIDs for enhanced analgesia
- Advantages:
- Minimal anti-inflammatory effect
- Low gastrointestinal risk
- Safe in pregnancy (first choice)
- Limitations:
- No anti-inflammatory effect
- Hepatotoxicity at high doses
- Less effective than ibuprofen as a sole agent for post-surgical dental pain
10. Combination Therapy: Ibuprofen + Paracetamol
The combination of ibuprofen and paracetamol represents one of the most significant advances in dental pain management in recent years.
10.1 Evidence Base
High-quality evidence has reshaped postoperative pain management in dentistry. A 2018 overview of systematic reviews in JADA found that ibuprofen 400 mg plus acetaminophen 1,000 mg provides superior analgesia.
10.2 Why Combination Therapy Works
Ibuprofen and paracetamol have complementary mechanisms of action:
- Ibuprofen works peripherally by reducing inflammation at the pain site.
- Paracetamol works centrally by raising the pain threshold in the CNS.
This dual action provides enhanced pain relief that is greater than the sum of their individual effects.
10.3 Clinical Evidence
- Ibuprofen, when used alongside acetaminophen, is more effective in relieving pain within the first hour after extraction than acetaminophen alone.
- Ibuprofen is superior to acetaminophen for managing post-extraction pain, and the combination of both drugs provides enhanced pain relief.
- The combination of paracetamol and ibuprofen is well-tolerated and effective for postoperative pain after surgical removal of mandibular third molars.
- The ibuprofen-acetaminophen combination resulted in quicker and sustained pain relief as well as fewer adverse effects such as nausea, dizziness, and constipation.
10.4 Recommended Dosing
| Component | Dose | Frequency |
|---|---|---|
| Ibuprofen | 200–400 mg | Every 6–8 hours |
| Paracetamol | 500–1,000 mg | Every 4–6 hours |
Important: Ensure total daily doses do not exceed 2,400 mg for ibuprofen and 3,000–4,000 mg for acetaminophen.
10.5 ADA Seal of Acceptance
The Advil Dual Action product (containing a combination of acetaminophen and ibuprofen) earned a first-in-category ADA Seal of Acceptance after demonstrating safety and efficacy in the temporary management of acute dental pain.
11. Opioids in Dental Pain
11.1 Current Recommendations
The evidence is clear: NSAIDs with or without acetaminophen are first-line therapy for managing acute dental pain. Opioids should be reserved for clinical situations when:
- First-line therapy is insufficient
- Contraindications to NSAIDs exist
- Pain is severe and not responding to non-opioid analgesics
11.2 Evidence Against Routine Opioid Use
- Evidence from 87 RCTs shows that NSAIDs—alone or combined with acetaminophen—are more effective for postoperative dental pain relief than opioids.
- NSAIDs are actually safer and more effective than opioids at reducing acute dental pain in people of all ages.
- Opioids are associated with significant risks: addiction, respiratory depression, and mental health issues.
11.3 When Opioids May Be Considered
The ADA guidelines suggest that in rare instances when post-visit pain control using NSAIDs in combination with acetaminophen proved inadequate, a low-dose opioid may be added for a maximum of three days.
Recommended opioid combinations (if used):
- 325 mg acetaminophen + 5–7.5 mg hydrocodone
- 325 mg acetaminophen + 5 mg oxycodone
11.4 Opioids to Avoid
Opioids should be avoided for patients taking:
- Gabapentinoids
- Central nervous system active medications
- Existing opioids
12. Corticosteroids
Corticosteroids can be valuable adjuncts in managing dental pain, particularly in postoperative settings.
12.1 Mechanism
Corticosteroids modulate inflammatory responses by:
- Inhibiting phospholipase A2
- Reducing prostaglandin synthesis
- Decreasing capillary permeability
- Suppressing immune cell migration
12.2 Clinical Evidence
- Evidence consistently demonstrates the clinical efficacy of corticosteroids—especially dexamethasone—in reducing postoperative edema, trismus, and pain, notably in third molar extractions, orthognathic surgeries, and facial fracture repairs.
- Corticosteroids were generally found to be more effective than NSAIDs in some studies.
- Low-dose methylprednisolone is statistically and clinically effective in reducing postoperative pain and swelling.
12.3 Clinical Use
Corticosteroids are not first-line treatment for mild to moderate dental pain. They may be considered for:
- Third molar surgery
- Severe inflammatory conditions
- Patients who cannot tolerate NSAIDs
- Adjunctive therapy in complex cases
12.4 Examples
- Dexamethasone: 4–8 mg orally or intravenously
- Methylprednisolone: 8 mg (low dose) for postoperative pain
- Prednisolone: May be used as premedication
13. Local Anesthetics
Local anesthetics provide immediate, profound pain relief and are essential for both dental procedures and temporary pain management.
13.1 Commonly Used Local Anesthetics
Most local anesthetics used in dental procedures belong to the amide group:
| Agent | Duration | Characteristics |
|---|---|---|
| Lidocaine 2% with 1:100,000 epinephrine | 60–90 minutes | Most commonly used; rapid onset |
| Articaine 4% with 1:100,000 epinephrine | 60–90 minutes | High lipid solubility; good bone penetration |
| Mepivacaine 2% | 60–90 minutes | No epinephrine option available |
| Bupivacaine 0.5% with 1:200,000 epinephrine | 180–240 minutes | Prolonged duration; useful for postoperative pain |
13.2 ADA Recommendations
For the temporary management of toothache prior to definitive dental treatment, the ADA suggests the use of a short-acting local anesthetic (e.g., 2% lidocaine plus 1:100,000 epinephrine or 4% articaine plus 1:100,000 epinephrine) for immediate pain relief.
13.3 Topical Anesthetics
Topical anesthetics such as benzocaine and lidocaine gel can provide temporary relief for superficial pain. Both 2% lignocaine jelly and benzocaine gel significantly reduce procedural tooth pain compared with placebo.
13.4 Long-Acting Local Anesthetics
Bupivacaine is particularly beneficial for postoperative pain management due to its prolonged duration of anesthesia, which is attributed to its high lipid solubility and strong protein-binding potential. Consider using local bupivacaine at closure to minimize postoperative pain.
14. Antibiotics in Dental Pain
A critical concept for BDS students: Antibiotics are not painkillers.
14.1 Current Guidelines
The ADA clinical practice guideline on antibiotic use for the urgent management of pulpal- and periapical-related dental pain and intraoral swelling recommends against using antibiotics for most pulpal and periapical conditions.
Key recommendations:
- For symptomatic irreversible pulpitis, symptomatic apical periodontitis, and localized acute apical abscess, the expert panel suggests dentists prescribe oral amoxicillin (500 mg, three times a day, with or without loading dose of 1,000 mg) ONLY when there are signs of spreading infection or systemic involvement.
- Antibiotic prescribing should shift from a “just in case” mentality to “only when absolutely necessary”.
14.2 When Antibiotics Are Indicated
- Signs of spreading infection (cellulitis, facial swelling)
- Systemic symptoms (fever, malaise)
- Immunocompromised patients
- Patients at risk of infective endocarditis (with appropriate prophylaxis)
14.3 Common Antibiotics in Dentistry
| Antibiotic | Dose | Indication |
|---|---|---|
| Amoxicillin | 500 mg TDS | First-line for odontogenic infections |
| Metronidazole | 400 mg TDS | Anaerobic infections; often combined with amoxicillin |
| Clindamycin | 150–300 mg QDS | Penicillin allergy |
| Cefalexin | 500 mg QDS | Nonsevere penicillin hypersensitivity |
14.4 Key Takeaway
Dental treatment (extraction, root canal, drainage) is the definitive management for toothache. Analgesics manage pain; antibiotics manage infection—not pain. Never prescribe antibiotics solely for pain relief.
15. Clinical Studies and Evidence Synthesis
15.1 Key Systematic Reviews and Meta-Analyses
- ADA Overview of Systematic Reviews (2018): Found that ibuprofen 400 mg plus acetaminophen 1,000 mg provides superior analgesia compared with either drug alone.
- Network Meta-Analysis (2026): The combination of an opioid with an NSAID ranked as the most effective strategy for managing moderate-to-severe pain after third molar surgery. However, this must be balanced against safety concerns.
- Endodontic Pain Meta-Analysis (2026): At 6–8 hours, diclofenac + acetaminophen provided the greatest pain reduction (MD: -6.28, 95% CI: -11.99 to -0.56), followed by Novafen and ibuprofen + acetaminophen.
- Cochrane Reviews: Consistently support NSAIDs, especially ibuprofen, as effective for postoperative dental pain. Paracetamol 1,000 mg provides safe and effective analgesia with minimal adverse effects following dental extraction (Level I evidence).
- Third Molar Surgery Evidence: The combination of paracetamol and ibuprofen is well-tolerated and effective for postoperative pain after surgical removal of mandibular third molars.
15.2 Comparative Efficacy
- Ibuprofen vs. Paracetamol: Ibuprofen is significantly more efficacious than paracetamol in the management of post-surgical dental pain.
- NSAIDs vs. Opioids: NSAIDs with or without acetaminophen provide superior pain relief with a more favorable safety profile compared with opioids.
- Combination vs. Monotherapy: The combination of ibuprofen and paracetamol provides enhanced pain relief compared with either drug alone.
15.3 Number Needed to Treat (NNT)
Cochrane data on NNTs in dental pain studies demonstrate that:
- NSAIDs have favorable NNTs for dental pain
- The combination of ibuprofen and paracetamol has a particularly favorable NNT
- Opioids generally have higher NNTs (less efficient) for dental pain
16. Drug Comparison Table
| Drug | Class | Pain Relief | Anti-inflammatory | Duration | GI Risk | Onset | Max Daily Dose |
|---|---|---|---|---|---|---|---|
| Ibuprofen | NSAID (non-selective) | Excellent | Excellent | 4–6 h | Moderate | 30 min | 2,400 mg |
| Paracetamol | Analgesic/Antipyretic | Good | Minimal | 4–6 h | Low | 30–60 min | 3,000–4,000 mg |
| Naproxen | NSAID (non-selective) | Excellent | Excellent | 8–12 h | Moderate | 1–2 h | 1,375–1,500 mg |
| Diclofenac | NSAID (non-selective) | Excellent | Excellent | 6–8 h | Moderate | 30–60 min | 150 mg |
| Ketorolac | NSAID (non-selective) | Very High | Excellent | 4–6 h | Higher | 30–60 min | 40 mg (≤5 days) |
| Celecoxib | NSAID (COX-2 selective) | Good | Good | 12–24 h | Lower | 1–2 h | 400 mg |
| Lidocaine | Local anesthetic | Immediate | None | 60–90 min | None | 1–2 min | Variable |
| Amoxicillin | Antibiotic | None | None | N/A | Low | N/A | 1,500 mg |
17. Adult and Pediatric Dosages
17.1 Adult Dosages (≥12 years)
| Drug | Recommended Dose | Frequency | Maximum Daily Dose |
|---|---|---|---|
| Ibuprofen | 200–400 mg | Every 6–8 hours | 2,400 mg |
| Paracetamol | 500–1,000 mg | Every 4–6 hours | 3,000–4,000 mg |
| Naproxen sodium | 440 mg | Twice daily | 1,375 mg |
| Diclofenac | 50 mg | Three times daily | 150 mg |
| Ketorolac | 10–20 mg | Every 4–6 hours | 40 mg (≤5 days) |
| Celecoxib | 100–200 mg | Once or twice daily | 400 mg |
17.2 Pediatric Dosages
Pediatric dosing must be weight-based:
| Drug | Dose | Frequency |
|---|---|---|
| Paracetamol | 10–15 mg/kg | Every 4–6 hours |
| Ibuprofen | 5–10 mg/kg | Every 6–8 hours |
Important considerations:
- Accurate, personalized dosing of paracetamol and ibuprofen is crucial for effective symptom management in children.
- For dental pain in children, an appropriate five-day regimen is either paracetamol (500 mg tablets, or 120 mg/5 ml or 250 mg/5 ml oral suspension), dose depending on age, up to four times daily.
- The combination of ibuprofen and acetaminophen at fixed doses appears to be a viable option for dental pain treatment in children, although further RCTs are needed.
18. Pregnancy and Lactation Considerations
18.1 First Trimester
- Paracetamol: The analgesic of choice during pregnancy. It is safe to take paracetamol when pregnant; adult dose is 2 tablets up to 4 times a day.
- NSAIDs: Should be avoided if possible. If necessary, use up to week 28 of pregnancy if clinically indicated.
18.2 Third Trimester
- NSAIDs: Contraindicated in the third trimester of pregnancy due to the risk of premature ductus arteriosus closure.
- Paracetamol: Remains the preferred option.
18.3 Lactation
- Paracetamol: Considered safe during breastfeeding.
- NSAIDs: Generally considered compatible with breastfeeding, but use the lowest effective dose for the shortest duration.
18.4 Codeine
Codeine may be used at any stage of pregnancy when stronger pain relief than paracetamol or NSAID is required. However, caution is advised due to variable metabolism and potential neonatal effects.
19. Contraindications
19.1 NSAID Contraindications
- Active peptic ulcer disease or history of upper gastrointestinal bleeding
- Severe renal impairment (chronic kidney disease)
- Severe hepatic impairment (chronic liver disease)
- Cardiovascular disease (increased risk of heart attack, heart failure, and stroke)
- Third trimester of pregnancy
- Hypersensitivity to aspirin or other NSAIDs
- Bleeding disorders or anticoagulation therapy
19.2 Paracetamol Contraindications
- Severe hepatic impairment
- Chronic alcohol use (increases hepatotoxicity risk)
19.3 Relative Contraindications (Use with Caution)
- History of gastrointestinal intolerance
- Asthma (NSAIDs may precipitate bronchospasm)
- Elderly patients (higher risk of adverse effects)
- Patients on anticoagulants, SSRIs, or methotrexate
20. Side Effects and Adverse Reactions
20.1 NSAIDs
| System | Adverse Effects |
|---|---|
| Gastrointestinal | Nausea, dyspepsia, ulceration, bleeding |
| Renal | Fluid retention, renal impairment |
| Cardiovascular | Increased risk of MI, stroke, hypertension |
| Hematological | Inhibition of platelet aggregation |
| Hepatic | Elevated liver enzymes (rare) |
| Hypersensitivity | Rash, angioedema, bronchospasm (in asthmatics) |
20.2 Paracetamol
| System | Adverse Effects |
|---|---|
| Hepatic | Hepatotoxicity at high doses (>4 g/day) |
| Renal | Nephrotoxicity (chronic high-dose use) |
| Hypersensitivity | Rash, rare anaphylaxis |
20.3 Opioids
| System | Adverse Effects |
|---|---|
| CNS | Drowsiness, dizziness, respiratory depression |
| Gastrointestinal | Constipation, nausea, vomiting |
| Psychological | Addiction, dependence, euphoria/dysphoria |
| Endocrine | Hormonal dysregulation |
20.4 Monitoring
For patients on NSAIDs, especially with prolonged use, monitor:
- Renal function
- Blood pressure
- Signs of GI bleeding
- Hepatic function
21. Drug Interactions
21.1 NSAID Interactions
NSAIDs have numerous interactions with other medications:
| Interacting Drug | Effect |
|---|---|
| Antihypertensives | Reduced antihypertensive efficacy |
| Anticoagulants (warfarin) | Increased bleeding risk |
| SSRIs | Increased bleeding risk |
| Methotrexate | Increased methotrexate toxicity |
| Lithium | Increased lithium levels |
| Aspirin | Reduced antiplatelet effect of aspirin |
| Fluconazole, Voriconazole | Increased plasma concentration of ibuprofen |
21.2 Paracetamol Interactions
- Alcohol: Increased risk of hepatotoxicity
- Warfarin: Enhanced anticoagulant effect with chronic high-dose paracetamol
- Anticonvulsants: Increased hepatotoxicity risk
21.3 Drug Combinations
- Ibuprofen + Paracetamol: No significant interaction; synergistic analgesia
- Naproxen + Acetaminophen: Can be taken together safely for most healthy adults; minimal direct interaction
21.4 General Precautions
- Review drug interactions prior to prescribing
- Screen patients for conditions requiring cautious use of NSAIDs
- Avoid combining multiple NSAIDs (no additional benefit, increased risk)
- Educate patients about potential interactions with over-the-counter medications
22. Clinical Case Scenarios
Case 1: Acute Irreversible Pulpitis
Presentation: A 28-year-old female presents with severe, spontaneous pain in the lower left first molar. Pain is worse at night and exacerbated by cold drinks. No swelling or systemic symptoms.
Diagnosis: Symptomatic irreversible pulpitis.
Management:
- Definitive treatment: Root canal treatment (referral to endodontist)
- Immediate pain management: Ibuprofen 400 mg every 6–8 hours OR ibuprofen 400 mg + paracetamol 500 mg every 6–8 hours
- Antibiotics: Not indicated (no signs of spreading infection)
- Patient education: Explain that analgesics are for temporary relief; definitive dental treatment is required
Rationale: This is inflammatory pain. NSAIDs directly address the inflammation. Antibiotics would be inappropriate and ineffective for pain relief.
Case 2: Post-Extraction Pain (Third Molar Surgery)
Presentation: A 22-year-old male undergoes surgical removal of impacted lower third molars. He experiences moderate to severe pain on the first postoperative day.
Management:
- First-line: Ibuprofen 400 mg + paracetamol 1,000 mg every 6–8 hours
- Alternative: Naproxen sodium 440 mg twice daily
- Local measures: Ice packs, rest, soft diet
- Rescue: If pain persists, consider adding low-dose opioid for a maximum of 3 days
- Avoid: Routine opioid prescription
Rationale: The ibuprofen-paracetamol combination provides superior analgesia with fewer adverse effects than opioids.
📋 Case 3: NSAID-Contraindicated Patient
Presentation: A 65-year-old female with a history of peptic ulcer disease presents with toothache from a carious upper premolar. She requires pain management before definitive treatment.
Management:
- First-line: Paracetamol 1,000 mg every 4–6 hours
- Alternative: Celecoxib 100–200 mg daily (if ulcer healed and GI risk considered acceptable)
- Definitive treatment: Dental restoration or extraction
- Avoid: Non-selective NSAIDs
Rationale: Paracetamol is the safest option for patients with GI contraindications to NSAIDs.
📋 Case 4: Spreading Dental Infection
Presentation: A 45-year-old male presents with severe toothache, facial swelling, trismus, and fever. The lower left second molar is tender to percussion.
Diagnosis: Acute apical abscess with spreading cellulitis.
Management:
- Immediate: Incision and drainage of abscess
- Antibiotics: Amoxicillin 500 mg three times daily for 5–7 days
- Analgesics: Ibuprofen 400 mg + paracetamol 500 mg
- Referral: Endodontic or surgical treatment
Rationale: Antibiotics are indicated because there are signs of spreading infection and systemic involvement. However, antibiotics are adjunctive to—not a replacement for—definitive dental treatment.
📋 Case 5: Pediatric Dental Pain
Presentation: A 6-year-old child (weight 20 kg) complains of toothache from a carious primary molar. No swelling or systemic signs.
Management:
- Paracetamol: 10–15 mg/kg = 200–300 mg every 4–6 hours
- Alternative: Ibuprofen 5–10 mg/kg = 100–200 mg every 6–8 hours
- Definitive treatment: Dental restoration or extraction
- Parent education: Accurate weight-based dosing is crucial
Rationale: Pediatric dosing must be weight-based. Paracetamol is often the first choice for children due to safety profile, but ibuprofen is also effective.
ادویات، بیماریوں، علاج، خوراک، مضر اثرات اور طبی معلومات کے لیے Learn about medicines, diseases, treatments, dosages, side effects, and medical information at ssthem.org.
References
1. Green VG, Polk DE, Turturro MA, Moore PA, Carrasco-Labra A. Evidence-based clinical practice guidelines for the management of acute dental pain. Am J Emerg Med. 2024;89:247-253.
2. American Dental Association. Evidence-Based Clinical Practice Guideline for the Temporary Pharmacologic Management of Acute Dental Pain: Toothache in Adolescents, Adults, and Older Adults. ADA Living Guideline Program, 2024.
3. American Dental Association. Oral Analgesics for Acute Dental Pain. Oral Health Topics, 2025.
4. Moore PA, Ziegler KM, Lipman RD, et al. Benefits and harms associated with analgesic medications used in the management of acute dental pain: An overview of systematic reviews. J Am Dent Assoc. 2018;149(4):256-265.
5. Lockhart PB, Tampi MP, Abt E, et al. Evidence-based clinical practice guideline on antibiotic use for the urgent management of pulpal- and periapical-related dental pain and intraoral swelling. J Am Dent Assoc. 2019;150(11):906-921.
6. Cochrane Review. Paracetamol 1000 mg provides safe and effective analgesia following dental extraction (Level I evidence).
7. Efficacy and safety of single-dose oral postoperative medications in reducing pain after endodontic treatment: a systematic review and meta-analysis. BMC Oral Health. 2026.
8. Management of pain with oral analgesia after extraction of lower third molars: a network meta-analysis of randomized controlled trials. 2026.
9. COX-2 selective nonsteroidal anti-inflammatory drugs: what is their place in managing dental pain? Australian Prescriber. 2025.
10. Use of corticosteroids in dental surgical procedures. Braz J Implantol Health Sci. 2025.
11. Local Anesthetic Drugs Used In Dentistry. StatPearls. 2025.
12. Review of Literatures: Physiology of Orofacial Pain in Dentistry. PMC. 2021.
13. Dental pain in children: pharmacological management. 2025.
14. Medicines and pregnancy. Waikato DHB. 2026.
15. Contraindications & cautions – analgesics. SDCEP Dental Prescribing.
16. NSAIDs have numerous interactions with other medications that are pertinent in dentistry.
The evidence-based answer to “What is the best medicine for tooth pain?” is clear: NSAIDs—particularly ibuprofen—are the first-line therapy for most dental pain. For moderate to severe pain, the combination of ibuprofen and paracetamol provides superior analgesia compared with either drug alone and performs as well as or better than opioids with fewer adverse effects. Antibiotics are not painkillers and should be reserved for cases with signs of spreading infection.
For BDS students, mastering this evidence-based approach is essential for providing safe, effective, and responsible pain management. The key principles to remember are:
- Treat the cause: Definitive dental treatment (restoration, root canal, extraction) is the ultimate solution.
- Choose the right analgesic: NSAIDs for inflammatory pain; paracetamol when NSAIDs are contraindicated; combination therapy for moderate to severe pain.
- Avoid unnecessary opioids: Non-opioid therapy is safer and equally or more effective.
- Reserve antibiotics for infection: Antibiotics treat infection, not pain.
- Consider the patient: Individualize treatment based on medical history, contraindications, and patient preferences.
By adhering to these evidence-based principles, dental professionals can optimize pain relief while minimizing risks and contributing to the broader public health goal of reducing opioid overprescription and antimicrobial resistance.
Disclaimer: This comprehensive clinical guide is intended for educational purposes only. It does not replace clinical judgment or individual patient assessment. Always follow local guidelines and individual patient factors when making treatment decisions. Consult drug interactions and current prescribing information before initiating therapy.
Last Updated: June 2026 | Version: 2.0 | Review Frequency: Annual review recommended
Facebook Copyright Issues Solution 2026
SSTHEM.COM – Learn World Religions, History & Educational Knowledge
·
Health & Beauty Tips
This article has been written with a focus on evidence-based medicine, clinical pharmacology, and practical application for dental students, residents, and practicing healthcare professionals. The content aligns with contemporary guidelines and antimicrobial stewardship principles.