Drug Absorption Explained 8 Key Factors & Mechanisms for Pharmacology Success
Drug Absorption in Pharmacology: A Comprehensive Clinical Guide 2026 | Drug Absorption Mechanisms, Factors Affecting Drug Absorption & Clinical Significance
Pharmacokinetics—the study of how the body affects a drug—rests upon four fundamental processes: absorption, distribution, metabolism, and excretion. Among these, drug absorption represents the most foundational principle, serving as the gateway through which therapeutic agents enter the systemic circulation and ultimately reach their sites of action.
The clinical significance of drug absorption cannot be overstated. A drug, regardless of its pharmacological potency, is therapeutically useless if it cannot be absorbed in sufficient quantities to achieve effective concentrations at its target site. The percentage of drug absorption varies considerably among different routes of administration—oral, subcutaneous, transdermal, intravenous, intramuscular, and others—each presenting unique challenges and opportunities for drug delivery.
The oral route remains the most common and preferred method of drug administration, owing to its convenience, high patient compliance, and cost-effectiveness. However, oral drug absorption is a remarkably complex process influenced by physicochemical properties of the drug (pKa, lipophilicity, solubility), pharmaceutical factors (dosage form design), and physiological conditions (gastrointestinal pH, gastric emptying rate, intestinal transit time, metabolic activity).
This comprehensive article examines drug absorption from its fundamental mechanisms through its clinical applications, providing healthcare professionals, students, and researchers with an evidence-based understanding of this cornerstone of pharmacotherapy.
1. What Is Drug Absorption?
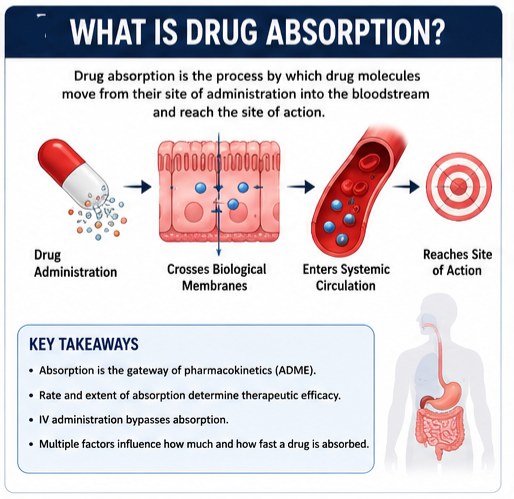 Drug absorption is the process by which drug molecules move from their site of administration into the bloodstream. More precisely, pharmacokinetic theory defines drug absorption as the transportation of the unmetabolized drug from the administration site to the body circulation system.
Drug absorption is the process by which drug molecules move from their site of administration into the bloodstream. More precisely, pharmacokinetic theory defines drug absorption as the transportation of the unmetabolized drug from the administration site to the body circulation system.
The speed of this process—the rate of drug absorption—and its completeness—the extent of drug absorption—are critical determinants of therapeutic efficacy. These parameters collectively determine how quickly a drug reaches effective concentrations and how much of the administered dose ultimately becomes available for pharmacological action.
For a drug to be absorbed, it must first be released from its pharmaceutical dosage form (tablet, capsule, solution, etc.) and then cross biological membranes to enter the systemic circulation. Unless administered intravenously, a drug must cross several semipermeable cell membranes before it reaches the systemic circulation.
Formal Definition
From a pharmacological standpoint, drug absorption can be formally defined as:
“The process by which an active drug ingredient or therapeutic moiety moves from its site of administration into the systemic circulation, thereby becoming available at the site of drug action to produce a pharmacological effect.”
This definition encompasses several critical elements:
- Site of administration: The anatomical location where the drug is introduced (oral cavity, gastrointestinal tract, muscle tissue, skin, etc.)
- Systemic circulation: The bloodstream, which serves as the transport medium for distributing drugs throughout the body
- Site of action: The specific receptor or target tissue where the drug exerts its therapeutic effect
The United States Food and Drug Administration (FDA) defines bioavailability—the measurable outcome of absorption—as “the rate and extent to which the active ingredient or active moiety is absorbed from a drug product and becomes available at the site of action.”
2. Historical Background
The scientific understanding of drug absorption has evolved considerably over the past century. The first edition of Goodman & Gilman’s The Pharmacological Basis of Therapeutics, published in 1941, helped organize the field of pharmacology, giving it intellectual validity and an academic identity. This seminal work established pharmacokinetics—including drug absorption—as a foundational discipline within pharmacology.
Early pharmacokinetic research focused on describing the time course of drug concentrations in the body using mathematical models. The development of the pH partition theory in the mid-20th century provided a mechanistic understanding of how drug ionization and environmental pH influence membrane permeability. This theory remains fundamental to predicting drug absorption behavior today.
The introduction of biopharmaceutics as a discipline in the 1960s and 1970s bridged the gap between the physical-chemical properties of drugs and their biological performance. The FDA’s formal introduction of the term bioavailability in regulatory guidance established drug absorption as a critical parameter in drug development and approval.
More recently, the Biopharmaceutics Classification System (BCS), developed by Amidon and colleagues, has provided a framework for predicting oral drug absorption based on solubility and permeability characteristics. This system has been adopted by regulatory agencies worldwide, including the FDA and the European Medicines Agency (EMA), to guide biowaiver decisions and streamline generic drug approvals.
3. Importance of Drug Absorption in Pharmacotherapy
The clinical importance of drug absorption manifests in several critical areas:
Therapeutic Efficacy
Drug absorption determines whether a medication can achieve therapeutic concentrations at its site of action. Inadequate absorption leads to subtherapeutic levels and treatment failure, while excessive absorption may result in toxicity.
Dosage Regimen Design
Understanding absorption characteristics—rate, extent, and variability—is essential for designing appropriate dosing intervals and routes of administration. Drugs with poor or variable absorption may require higher doses, alternative formulations, or different routes of administration.
Bioequivalence Assessment
The FDA considers two drug products bioequivalent if “their bioavailabilities (rate and extent of drug absorption) after administration in the same molar dose lie within acceptable predefined limits.” This principle underpins the generic drug approval process, ensuring that generic products perform comparably to their brand-name counterparts.
Individualized Therapy
Factors affecting drug absorption—including age, disease states, genetic polymorphisms, and concomitant medications—must be considered when tailoring therapy to individual patients. This is particularly important in special populations such as children, the elderly, and pregnant women.
Drug Development
Pharmaceutical companies invest considerable resources in optimizing drug absorption through formulation strategies, prodrug design, and selection of appropriate routes of administration. The Biopharmaceutics Classification System (BCS) has become an essential tool in this process.
4. Anatomy and Physiology Relevant to Drug Absorption
Understanding drug absorption requires familiarity with the anatomical structures and physiological processes that drugs encounter on their journey to the systemic circulation.
Cell Membranes as Biological Barriers
Regardless of the absorption site, a drug must cross cell membranes to reach the systemic circulation. Cell membranes are biologic barriers that selectively inhibit the passage of drug molecules. They are composed primarily of a bimolecular lipid matrix, which determines membrane permeability characteristics.
The Gastrointestinal Tract
For orally administered drugs, the gastrointestinal (GI) tract presents a complex series of anatomical and physiological barriers:
| GI Segment | pH Range | Residence Time | Key Features |
|---|---|---|---|
| Mouth | ~6.5 | Seconds | Salivary enzymes, limited surface area |
| Stomach | 1.0–3.0 | 1–3 hours | Gastric acid, pepsin, limited absorption area |
| Duodenum | 4.0–5.5 | 30–40 minutes | Bile salts, pancreatic enzymes |
| Jejunum | 5.5–7.0 | 1.5–2 hours | Large surface area, major absorption site |
| Ileum | 7.0–7.5 | 5–7 hours | Vitamin B12 absorption, bile salt reabsorption |
| Colon | 6.0–6.7 | 16–34 hours | Bacterial metabolism, limited absorption |
Data compiled from multiple sources
The small intestine—particularly the duodenum and jejunum—represents the primary site of drug absorption due to its enormous surface area (approximately 200 m²) and highly permeable membrane.
Blood Flow
Regional blood flow significantly influences drug absorption. Well-perfused tissues (such as the small intestine) absorb drugs more rapidly than poorly perfused tissues (such as subcutaneous fat). Changes in splanchnic blood flow—which can occur in shock, heart failure, or with certain medications—can substantially alter drug absorption.
5. Mechanisms of Drug Absorption
Drugs cross biological membranes through several distinct mechanisms. Understanding these mechanisms is essential for predicting and optimizing drug absorption.
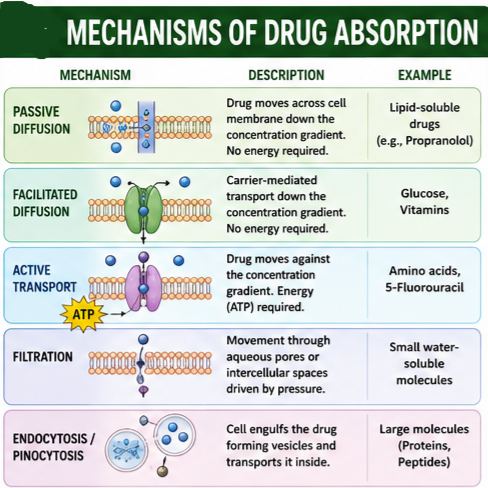
5.1 Passive Diffusion
Passive diffusion is the most common mechanism of drug absorption. In this process, drug molecules move according to the concentration gradient—from a region of higher concentration to one of lower concentration—until equilibrium is reached.
The rate of passive diffusion is described by Fick’s Law of Diffusion, which states that diffusion rate is directly proportional to:
- The concentration gradient across the membrane
- The molecule’s lipid solubility
- The surface area available for absorption
- The membrane permeability coefficient
- Inversely proportional to membrane thickness
Passive diffusion occurs in two environments:
- Aqueous Diffusion: Occurs in the aqueous compartment of the body, such as interstitial space, or through aqueous pores in the endothelium of blood vessels. Drugs bound to albumin or large plasma proteins cannot permeate most aqueous pores.
- Lipid Diffusion: Occurs through the lipid compartment of the body. This is considered the most critical factor for drug permeability due to the greater number of lipid barriers separating the body’s compartments. Because the cell membrane is lipoid, lipid-soluble drugs diffuse most rapidly.
Small molecules tend to penetrate membranes more rapidly than larger ones.
5.2 Facilitated Diffusion
Facilitated diffusion is a carrier-mediated transport process that, like passive diffusion, moves drugs down a concentration gradient without energy expenditure. However, it differs from passive diffusion in that it:
- Requires a specific carrier protein
- Exhibits saturability (carrier capacity is limited)
- Shows structural specificity (only drugs resembling the natural substrate are transported)
- Can be competitively inhibited
5.3 Active Transport
Active transport is an energy-consuming process that moves drugs against a concentration gradient. Key characteristics include:
- Requires energy (ATP)
- Moves drugs from low to high concentration
- Exhibits saturability and structural specificity
- Can be inhibited by metabolic poisons
Active transport is essential for gastrointestinal absorption and renal and biliary excretion of many drugs. This process facilitates the absorption of some lipid-insoluble drugs that mimic natural physiological metabolites, such as 5-fluorouracil from the GI tract.
5.4 Filtration
Filtration is the passage of drugs through aqueous pores or intercellular spaces driven by hydrostatic or osmotic pressure. This mechanism is primarily important for:
- Small water-soluble molecules (molecular weight < 100-200 Da)
- Drugs in the glomerulus of the kidney
- Drugs crossing capillary endothelium
5.5 Endocytosis and Pinocytosis
Endocytosis and pinocytosis involve the engulfment of extracellular material by the cell membrane, forming vesicles that transport the material into the cell. These processes are relatively unimportant for most drugs but may be relevant for:
- Very large molecules (proteins, peptides)
- Particulate matter
- Some vitamins (e.g., vitamin B12)
6. Physicochemical Properties Affecting Drug Absorption
 The physicochemical properties of a drug profoundly influence its absorption characteristics. These properties determine whether a drug can cross biological membranes and how efficiently it does so.
The physicochemical properties of a drug profoundly influence its absorption characteristics. These properties determine whether a drug can cross biological membranes and how efficiently it does so.
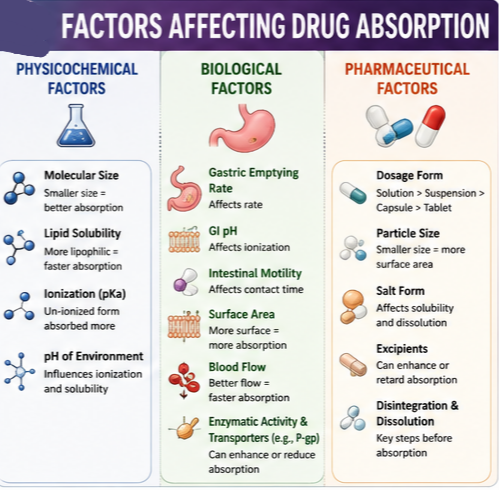
6.1 Molecular Size
Small molecules tend to penetrate membranes more rapidly than larger ones. Most drugs have molecular weights between 200 and 1000 Da, which allows them to cross biological membranes. Larger molecules (such as proteins and peptides) generally have poor membrane permeability and require specialized delivery systems.
6.2 Lipid Solubility
Lipid solubility (lipophilicity) is perhaps the most important determinant of passive diffusion across cell membranes. Because cell membranes are composed of a lipid bilayer, lipid-soluble drugs diffuse most rapidly.
The partition coefficient (log P) quantifies a drug’s relative affinity for lipid versus aqueous environments. Drugs with higher log P values (more lipophilic) generally show better membrane permeability, though excessively high lipophilicity can reduce aqueous solubility and impair dissolution.
6.3 Ionization and pKa
Most drugs are weak organic acids or bases, existing in both ionized and un-ionized forms in an aqueous environment. The un-ionized form is usually lipid soluble (lipophilic) and diffuses readily across cell membranes. The ionized form has low lipid solubility (but high water solubility—i.e., hydrophilic) and high electrical resistance, and thus cannot penetrate cell membranes easily.
The proportion of the un-ionized form present—and thus the drug’s ability to cross a membrane—is determined by the environmental pH and the drug’s pKa (acid dissociation constant).
The pKa is the pH at which concentrations of ionized and un-ionized forms are equal. The relationship between pH and ionization is described by the Henderson-Hasselbalch equation:
- For weak acids: pH = pKa + log ([ionized]/[un-ionized])
- For weak bases: pH = pKa + log ([un-ionized]/[ionized])
6.4 pH Partition Theory
The pH partition theory explains how drug absorption is influenced by gastrointestinal pH. Key principles include:
- For weak acids: When the pH is lower than the pKa, the un-ionized form predominates. Thus, in gastric fluid (pH 1.4), a weak acid with a pKa of 4.4 exists predominantly in the un-ionized form (ratio 1000:1), favoring diffusion through the gastric mucosa.
- For weak bases: When the pH is lower than the pKa, the ionized form predominates. Thus, in gastric fluid (pH 1.4), a weak base with a pKa of 4.4 exists predominantly in the ionized form.
Theoretically, weakly acidic drugs (e.g., aspirin) are more readily absorbed from an acid medium (stomach) than are weakly basic drugs (e.g., quinidine). However, whether a drug is acidic or basic, most absorption occurs in the small intestine because the surface area is larger and membranes are more permeable.
7. Biological Factors Affecting Drug Absorption
Patient-specific biological factors can significantly alter drug absorption, leading to interindividual variability in therapeutic response.
Gastric Emptying Rate
The rate at which the stomach empties its contents into the small intestine influences the rate of drug absorption. Factors that delay gastric emptying (e.g., fatty meals, anticholinergic drugs, opiates) may slow drug absorption, while factors that accelerate gastric emptying (e.g., metoclopramide, fasting) may hasten absorption.
Intestinal Motility
Intestinal motility affects the residence time of drugs in the small intestine, the primary site of absorption. Increased motility (e.g., in diarrhea) may reduce absorption by decreasing contact time, while decreased motility (e.g., in constipation, with anticholinergic drugs) may increase absorption.
Surface Area
The vast absorptive surface area of the small intestine—created by villi and microvilli—makes it the primary site of drug absorption. Conditions that reduce absorptive surface area (e.g., celiac disease, short bowel syndrome, surgical resection) can significantly impair drug absorption.
Blood Flow
Regional blood flow determines the rate at which absorbed drug is carried away from the absorption site. Increased blood flow maintains a concentration gradient favoring continued absorption, while decreased blood flow (e.g., in shock, heart failure) can slow or impair absorption.
Gastrointestinal pH
Gastrointestinal pH varies along the GI tract and influences drug ionization and solubility. Altered gastric pH (e.g., from proton pump inhibitors, H2-receptor antagonists, achlorhydria in the elderly) can affect the absorption of pH-dependent drugs.
Enzymatic Activity
The GI tract contains numerous enzymes that can metabolize drugs before absorption. The intestinal wall contains cytochrome P450 enzymes (particularly CYP3A4) and other metabolic enzymes that contribute to first-pass metabolism.
Efflux Transporters
P-glycoprotein (P-gp) and other efflux transporters actively pump drugs out of intestinal epithelial cells back into the intestinal lumen, limiting drug absorption. This mechanism significantly affects the bioavailability of many drugs, including digoxin, cyclosporine, and morphine.
8. Pharmaceutical Factors Affecting Drug Absorption
The formulation and manufacturing of drug products profoundly influence drug absorption.
Dosage Form
Different dosage forms release drug at different rates:
- Solutions: Rapidly absorbed (drug already in solution)
- Suspensions: Absorbed after dissolution
- Capsules: Absorbed after shell dissolution and drug dissolution
- Tablets: Absorbed after disintegration and drug dissolution
- Controlled-release formulations: Designed to release drug slowly over time
Disintegration and Dissolution
Regardless of the route of administration, drugs must be in solution to be absorbed. Thus, solid dosage forms (e.g., tablets) must be able to disintegrate and deaggregate.
Dissolution rate is often the rate-limiting step in drug absorption, particularly for poorly soluble drugs. The Noyes-Whitney equation describes dissolution rate:
dC/dt = k × A × (Cs – C)
Where: dC/dt = dissolution rate, k = dissolution rate constant, A = surface area of the solid, Cs = saturation solubility of the drug, C = concentration of drug in solution
Particle Size
Reduced particle size increases surface area, enhancing dissolution rate and absorption. This principle is exploited in the formulation of micronized and nanocrystal drug products.
Salt Form
The salt form of a drug can significantly influence its solubility and dissolution rate. For example, sodium salts of weak acids are generally more water-soluble than the free acid form.
Crystal Form
Different polymorphs (crystal forms) of the same drug can have different solubility and dissolution characteristics. The most stable polymorph is usually the least soluble.
Excipients : Inactive ingredients (excipients) in drug formulations can affect drug absorption through various mechanisms:
- Enhancing or retarding dissolution
- Affecting gastrointestinal motility
- Chelating or binding the drug
- Altering gastrointestinal pH
9. Drug Absorption by Route of Administration
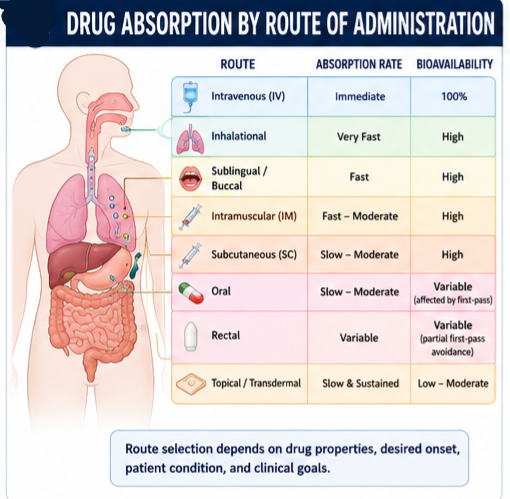
The route of administration determines the rate, extent, and reliability of drug absorption.
| Route | Advantages | Disadvantages | Absorption Characteristics |
|---|---|---|---|
| Oral | Convenient, non-invasive, economical | Variable absorption, first-pass metabolism | Slow to moderate, depends on GI factors |
| Sublingual | Rapid, bypasses first-pass | Limited to small lipophilic drugs | Fast, high bioavailability |
| Buccal | Bypasses first-pass, sustained delivery | Limited dose, taste issues | Moderate to fast |
| Rectal | Partial bypass of first-pass | Variable absorption, patient acceptability | Variable |
| Intramuscular (IM) | Rapid, avoids first-pass, reliable | Invasive, pain, requires trained personnel | Fast to moderate |
| Intravenous (IV) | Immediate, 100% bioavailability | Invasive, risk of infection, cannot be recalled | Absorption bypassed (immediate) |
| Subcutaneous (SC) | Avoids first-pass, sustained release | Variable absorption, limited volume | Slow to moderate |
| Inhalational | Rapid, avoids first-pass | Requires specialized device, technique-dependent | Very fast |
| Topical | Local delivery, avoids first-pass | Limited penetration, variable absorption | Slow, limited systemic absorption |
| Transdermal | Sustained delivery, avoids first-pass | Limited to small lipophilic drugs, skin irritation | Slow, sustained |
10. First-Pass Metabolism
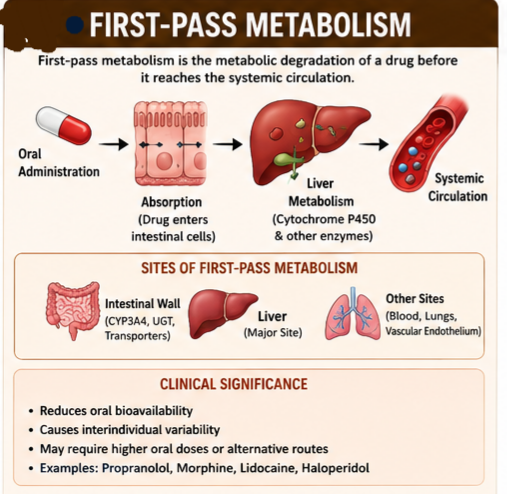
First-pass metabolism (also called presystemic metabolism) is the metabolic degradation of a drug before it reaches the systemic circulation. For orally administered drugs, this occurs in two primary sites:
Intestinal First-Pass Metabolism
After oral administration, the drug passes through the intestinal epithelium, where it may be metabolized by:
- Cytochrome P450 enzymes (particularly CYP3A4)
- Phase II conjugation enzymes (glucuronosyltransferases, sulfotransferases)
- Efflux transporters (P-glycoprotein)
Hepatic First-Pass Metabolism
After absorption from the intestine, the drug is carried via the portal vein to the liver, where it may undergo extensive metabolism before reaching the systemic circulation.
The liver is usually assumed to be the major site of first-pass metabolism, but other potential sites include the gastrointestinal tract, blood, vascular endothelium, and lungs.
Clinical Significance
First-pass metabolism has important clinical implications:
- Reduced bioavailability: Drugs subject to extensive first-pass metabolism have low oral bioavailability
- Interindividual variability: First-pass metabolism can vary considerably between patients
- Dose adjustment: Higher oral doses may be required compared to parenteral doses
- Route selection: Alternative routes (sublingual, buccal, rectal, parenteral) may be chosen to bypass first-pass metabolism
Examples
- Propranolol: 75–85% metabolized during first pass; oral bioavailability ~26%
- Haloperidol: Oral bioavailability ~60% due to extensive first-pass metabolism
- Morphine: Significant first-pass metabolism; oral bioavailability ~30%
- Lidocaine: Extensive first-pass metabolism; not used orally
11. Bioavailability
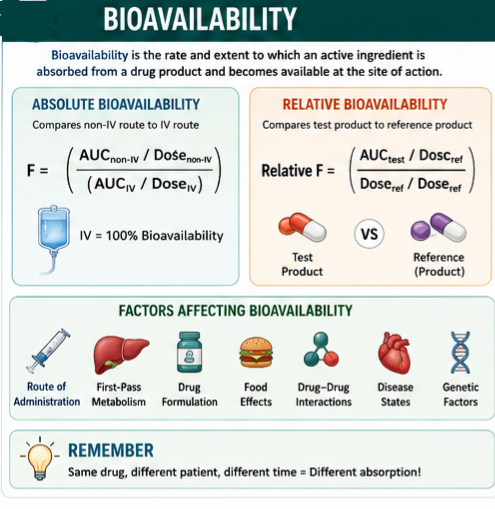
Bioavailability is one of the most important concepts in clinical pharmacokinetics. It is defined as “the rate and extent to which the active ingredient or active moiety is absorbed from a drug product and becomes available at the site of action.”
Absolute Bioavailability
Absolute bioavailability (F) compares the bioavailability of a drug after non-intravenous administration to that after intravenous administration:
F = (AUCnon-IV / Dosenon-IV) / (AUCIV / DoseIV)
Where AUC = area under the plasma concentration-time curve.
Relative Bioavailability
Relative bioavailability compares the bioavailability of two formulations of the same drug (e.g., generic vs. brand):
Relative F = (AUCtest / Dosetest) / (AUCreference / Dosereference)
Factors Affecting Bioavailability
- Route of administration: IV = 100%; other routes < 100%
- First-pass metabolism: Reduces bioavailability
- Drug formulation: Affects dissolution and absorption
- Food effects: Can increase or decrease bioavailability
- Drug interactions: Can alter absorption or metabolism
- Disease states: Can affect GI function, blood flow, metabolism
- Genetic factors: Polymorphisms in metabolizing enzymes and transporters
12. Drug–Food Interactions Affecting Absorption
Food can significantly affect drug absorption through multiple mechanisms.
Mechanisms of Food Effects
- Delayed gastric emptying: Fatty meals slow gastric emptying, delaying drug absorption
- Altered gastrointestinal pH: Food can buffer gastric acid, affecting drug ionization
- Competition for transporters: Food components may compete for absorption
- Chelation/complex formation: Food components (e.g., calcium, iron) can bind drugs
- Increased blood flow: Meals increase splanchnic blood flow, potentially enhancing absorption
- Altered dissolution: Food can affect drug dissolution and solubility
| Drug | Food Effect | Mechanism |
|---|---|---|
| Tetracycline | Decreased absorption | Chelation with calcium, iron |
| Griseofulvin | Increased absorption | Enhanced dissolution with fatty meal |
| Isoniazid | Decreased absorption | Competition for absorption |
| Levothyroxine | Decreased absorption | Binding to food components |
| Itraconazole | Increased absorption | Enhanced dissolution with acidic beverage |
Clinical Implications
- Timing of administration: Some drugs should be taken with food (to enhance absorption or reduce GI irritation); others should be taken on an empty stomach
- Consistency: Patients should be counseled to take medications consistently with respect to meals
- Specific foods: Patients taking medications with known food interactions should avoid specific foods (e.g., grapefruit juice with statins)
13. Special Populations: Pediatric, Geriatric & Pregnancy
Pediatric Drug Absorption
Drug absorption in children differs from adults due to developmental changes in gastrointestinal physiology and anatomy.
- Gastric pH: Neonates have higher gastric pH (less acidic) due to limited acid secretion, which can affect drug ionization and absorption
- Gastric emptying: In infants < 3 months, gastric emptying and intestinal motility are slowed
- Intestinal surface area: Larger relative to body weight in infants
- Intestinal enzymes: Young infants have reduced intestinal enzyme activity
- Transdermal absorption: Enhanced in neonates and young infants
Geriatric Drug Absorption
Age-related changes in gastrointestinal function can alter drug absorption in older adults:
- Gastric pH: Increased due to reduced acid secretion or use of acid-suppressing medications
- Gastric emptying: Slowed
- Intestinal surface area: Decreased
- Splanchnic blood flow: Reduced
- GI motility: Generally decreased
Despite age-related changes, changes in drug absorption tend to be clinically inconsequential for most drugs.
Drug Absorption During Pregnancy
Pregnancy induces profound physiological changes that can alter drug absorption and pharmacokinetics:
- Gastrointestinal: Delayed gastric emptying, reduced gastric acid secretion, decreased GI motility, increased gastric pH
- Cardiovascular: Increased cardiac output, increased splanchnic blood flow, expanded plasma volume
- Other: Increased body weight and fat, altered plasma protein binding, changes in drug-metabolizing enzyme activity
14. Clinical Examples (کلینیکل مثالیں)
Example 1: Propranolol
Propranolol is a beta-blocker with significant first-pass metabolism. Approximately 75–85% is metabolized by the liver before reaching the systemic circulation, resulting in an oral bioavailability of approximately 26%.
- Oral doses are much higher than intravenous doses
- Significant interindividual variability in response
- Alternative routes may be considered to bypass first-pass metabolism
Example 2: Clopidogrel
Clopidogrel is an antiplatelet drug whose absorption can be affected by gastric pH. Decreased gastric pH from proton pump inhibitors (PPIs) can reduce clopidogrel absorption and AUC.
- Avoid concomitant use of PPIs with clopidogrel when possible
- If PPI use is necessary, consider alternative antiplatelet therapy
Example 3: Morphine
Morphine is a substrate for P-glycoprotein, which affects its intestinal absorption and bioavailability.
- P-glycoprotein inhibitors can increase morphine absorption and effects
- Genetic polymorphisms in P-glycoprotein may contribute to variability in morphine response
15. Recent Research and Advances
Finite Absorption Time (F.A.T.) Concept
Recent analysis of oral drug absorption data based on the finite absorption time (F.A.T.) concept and physiologically based finite-time pharmacokinetic (PBFTPK) models has provided a better physiologically sound description of oral drug absorption.
Nanotechnology-Based Delivery Systems
Various strategies at the microscale/nanoscale have been developed to improve oral absorption of therapeutics:
- Nanocrystal formulations: To improve solubility and bioavailability of BCS class II drugs
- Lipid nanoparticles: To enhance intestinal uptake and pharmacokinetic profiles
- Transporter-mediated absorption: Targeting GI transporters/receptors to enhance absorption
Physiologically-Based Pharmacokinetic (PBPK) Modeling
The applications of PBPK absorption modeling and simulation have been expanding in recent years for both new drug and generic drug development. These models can predict drug absorption in special populations (pediatric, geriatric, pregnant) and under various disease states.
16. Key Takeaways (خلاصہ اور اہم نکات)
- Drug absorption is the transportation of the unmetabolized drug from the administration site to the systemic circulation
- Passive diffusion is the most common mechanism of drug absorption
- The un-ionized form of a drug is lipid-soluble and diffuses readily across cell membranes; the ionized form is hydrophilic and cannot penetrate membranes easily
- Most drugs are weak acids or bases; their absorption is influenced by pH and pKa
- The small intestine is the primary site of drug absorption due to its enormous surface area
- First-pass metabolism can significantly reduce the bioavailability of orally administered drugs
- Bioavailability is the rate and extent to which a drug is absorbed and becomes available at the site of action
- Route of administration determines the rate, extent, and reliability of drug absorption
- Drug–food and drug–drug interactions can significantly alter drug absorption
- Special populations (pediatric, geriatric, pregnant, critically ill) may have altered drug absorption requiring dose adjustments and monitoring
Question : What is drug absorption in pharmacology? (دوائی کا جذب کیا ہے؟)
Question : How are drugs absorbed into the body? (دوائیں جسم میں کیسے جذب ہوتی ہیں؟)
Question : What is the most common mechanism of drug absorption? (دوائیوں کے جذب کا سب سے عام طریقہ کون سا ہے؟)
Question : Why must drugs be in solution to be absorbed? (دوائیوں کو جذب ہونے کے لیے محلول میں کیوں ہونا چاہیے؟)
Question : What is the difference between rate and extent of absorption? (جذب کی شرح اور حد میں کیا فرق ہے؟)
Question : What factors affect drug absorption? (دوائیوں کے جذب کو کون سے عوامل متاثر کرتے ہیں؟)
Question : What is pH partition theory? (پی ایچ پارٹیشن تھیوری کیا ہے؟)
Question : Why is IV administration said to bypass absorption? (IV استعمال کو جذب کو نظرانداز کرنے والا کیوں کہا جاتا ہے؟)
Question : Why is oral absorption variable? (زبانی جذب متغیر کیوں ہے؟)
Question : What is bioavailability? (بائیو دستیابی کیا ہے؟)
Question : What is first-pass metabolism? (فرسٹ پاس میٹابولزم کیا ہے؟)
Question : Why does oral propranolol have low bioavailability? (زبانی پروپرانولول کی بائیو دستیابی کم کیوں ہے؟)
Question : How does food affect drug absorption? (خوراک دوائی کے جذب کو کیسے متاثر کرتی ہے؟)
Question : How do diseases affect drug absorption? (بیماریاں دوائی کے جذب کو کیسے متاثر کرتی ہیں؟)
Question : How does drug absorption differ in children? (بچوں میں دوائی کا جذب کیسے مختلف ہوتا ہے؟)
Question : Does drug absorption change with age? (کیا دوائی کا جذب عمر کے ساتھ بدلتا ہے؟)
Question : What is the role of P-glycoprotein in drug absorption? (دوائی کے جذب میں P-glycoprotein کا کیا کردار ہے؟)
Question : How are generic drugs approved? (عام دوائیں کیسے منظور ہوتی ہیں؟)
Question: What is the Biopharmaceutics Classification System (BCS)? (بائیو فارماسیوٹیکل درجہ بندی کا نظام کیا ہے؟)
Question: What are bioequivalence studies? (بائیو ایکویولینس اسٹڈیز کیا ہیں؟)
Drug absorption is a fundamental concept in pharmacology that underpins the entire field of pharmacotherapy. Understanding the mechanisms, factors, and clinical implications of drug absorption is essential for healthcare professionals to optimize drug therapy and improve patient outcomes.
From the simple diffusion of lipid-soluble molecules across cell membranes to the complex interplay of transporters, enzymes, and physiological factors, drug absorption represents a remarkable example of the intricate relationship between drugs and the human body.
Remember: The success of pharmacotherapy depends not only on the pharmacological properties of the drug but also on its ability to reach the site of action in adequate concentrations. A thorough understanding of drug absorption principles empowers clinicians to make informed decisions about drug selection, dosing, and route of administration.
As research continues to advance our understanding of drug absorption through PBPK modeling, nanotechnology, and personalized medicine approaches, the future holds promise for more effective and tailored drug therapy for all patients.
References (حوالہ جات)
Major Pharmacology Textbooks
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics. 13th Edition. New York: McGraw-Hill.
- Katzung BG, Vanderah TW. Basic & Clinical Pharmacology. 15th Edition. New York: McGraw-Hill.
- Rang HP, Dale MM, Ritter JM, Flower RJ, Henderson G. Rang & Dale’s Pharmacology. 9th Edition. Elsevier.
Regulatory and Clinical References
- FDA. M9 Biopharmaceutics Classification System-Based Biowaivers. Guidance Document. May 2021.
- FDA. Bioavailability Studies Submitted in NDAs or INDs – General Considerations. Guidance Document. 2022.
- Le J, Vivian EM. Drug Absorption. Merck Manual Professional Edition. November 2024.
- WHO. Bioavailability and Bioequivalence Studies. World Health Organization.
Peer-Reviewed Literature
- Almukainzi M, et al. Drug Absorption. In: StatPearls. Treasure Island (FL): StatPearls Publishing. 2024.
- New Drug Delivery Systems for Stable Oral Absorption: Theory, Strategies, and Applications. Biological & Pharmaceutical Bulletin. 2024;47(11):1797-1803.
- Enhancing Oral Drug Absorption: Overcoming Physiological and Pharmaceutical Barriers for Improved Bioavailability. AAPS PharmSciTech. 2024.
- Oral Absorption Basics: Pathways and Physicochemical and Biological Factors Affecting Absorption. ScienceDirect. 2017.
Additional Resources
- British National Formulary (BNF). Provides prescribing information and guidance on drug administration.
- European Medicines Agency (EMA). Guidelines on the investigation of bioequivalence.
- FDA. Bioavailability and Bioequivalence Requirements. 21 CFR Part 320.
(Disclaimer): یہ تعلیمی مواد صرف معلوماتی مقاصد کے لیے تیار کیا گیا ہے تاکہ فارماکولوجی میں دوائیوں کے جذب (Drug Absorption) کے بارے میں سمجھ بوجھ بڑھائی جا سکے۔ یہ کسی بھی قسم کی طبی مشاورت، تشخیص یا علاج کا متبادل نہیں ہے۔ کسی بھی دوائی کا استعمال کرنے سے پہلے ہمیشہ کسی مستند معالج یا فارماسسٹ سے مشورہ کریں۔ اس مضمون میں دی گئی معلومات تازہ ترین سائنسی تحقیقات اور مستند طبی حوالوں پر مبنی ہے تاہم ادویات کے استعمال سے متعلق کوئی بھی فیصلہ کرنے سے پہلے اپنے معالج سے ضرور مشورہ کریں۔
آخری اپ ڈیٹ: جولائی 2026 | ورژن: 2.0 | نظرثانی کی مدت: سالانہ نظرثانی تجویز کردہ
This educational content is for informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always consult your physician or pharmacist before taking any medication.