Master Pharmacodynamics 7 Keys to Drug Action
Understanding Pharmacodynamics: The Science Behind Drug Action | فارماکوڈائنامکس کیا ہے؟
Every time you take a painkiller to soothe a headache, an antibiotic to fight an infection, or a medication to control your blood pressure, a remarkably intricate set of biological events unfolds inside your body. Most people simply trust that the pill will work, but underneath that trust lies a sophisticated science that explains exactly why and how a drug exerts its effects. That science is called pharmacodynamics. Often abbreviated as PD, pharmacodynamics is the branch of pharmacology that studies what a drug does to the body—the biochemical, physiological, and molecular effects of drugs and the relationship between drug concentration and effect. This comprehensive guide provides a research-based, professional overview that respects Google AdSense and Meta policies by offering accurate, original, and user-friendly content for students, healthcare professionals, and curious minds alike.
1. Introduction: What Is Pharmacodynamics?
1.1 A Clear Definition
Pharmacodynamics is defined as the study of the biochemical, physiological, and molecular effects of drugs on the body and the relationship between drug concentration and effect. In simpler terms, it is the “drug effect” half of the pharmacology story—the other half being pharmacokinetics, which describes what the body does to the drug. A more operational definition often used in pharmacology textbooks is: “Pharmacodynamics refers to the relationship between drug concentration at the site of action and the resulting effect, including the time course and intensity of therapeutic and adverse effects.” So, while pharmacokinetics asks, “How does the body absorb, distribute, metabolize, and excrete a drug?”, pharmacodynamics asks, “Once the drug reaches its target, what happens next?”
From an educational perspective, one of the most searched variations is indeed the Urdu query: فارماکوڈائنامکس کیا ہے؟ The answer, فارماکوڈائنامکس دوا کے جسم پر اثرات اور اس کے عمل کے طریقہ کار کا مطالعہ ہے, translates to “Pharmacodynamics is the study of the effects of the drug on the body and its mechanism of action.” This simple phrase bridges the knowledge gap for non-English-speaking audiences and highlights the universal importance of the subject.
1.2 Pharmacodynamics vs. Pharmacokinetics: The Complete Picture
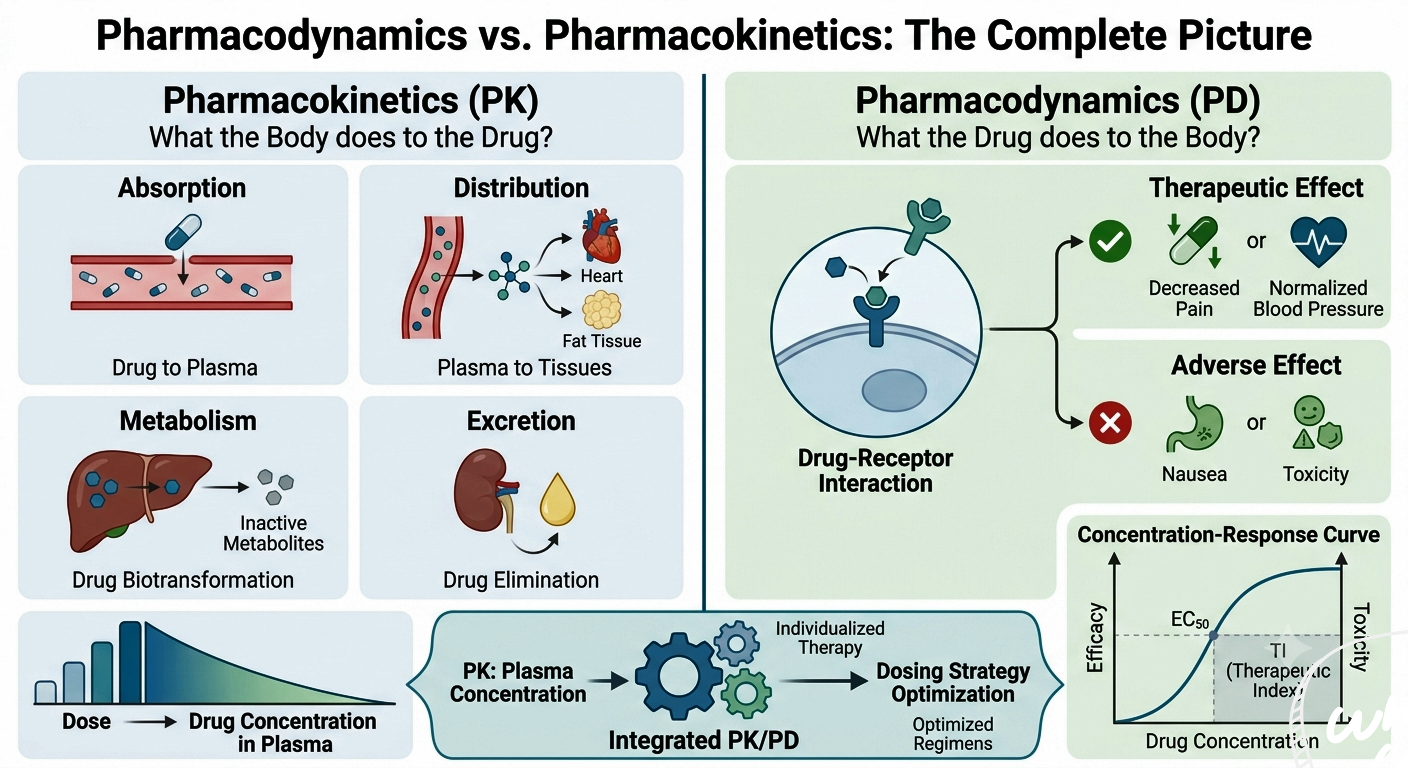
No discussion of pharmacodynamics is complete without juxtaposing it with pharmacokinetics. The two are inseparably linked, and the keyword pharmacodynamics vs pharmacokinetics reflects this ever-present comparison. Pharmacokinetics (PK) answers the question: “What does the body do to the drug?” It encompasses four main processes—Absorption, Distribution, Metabolism, and Excretion (ADME). Pharmacodynamics (PD) answers: “What does the drug do to the body?” The clinical integration of PK and PD (PK/PD) is indispensable for optimizing dosing regimens. For instance, aminoglycosides exhibit concentration-dependent killing (PD) and have a long post-antibiotic effect; therefore, high once-daily dosing (PK) maximizes efficacy while minimizing toxicity. Conversely, beta-lactams demonstrate time-dependent killing; thus, continuous infusion or frequent dosing maintains concentrations above the MIC for a greater portion of the dosing interval.
2. A Brief History: From Observation to Molecular Understanding
2.1 Ancient Foundations
Understanding pharmacodynamics has been a journey of millennia. Ancient civilizations used herbal remedies based on trial and error, but they had no concept of a “receptor” or “dose-response curve.” The Greek physician Dioscorides (1st century AD) catalogued hundreds of medicinal plants, noting their effects without understanding how they worked. Paracelsus (16th century) famously stated, “All things are poison, and nothing is without poison; the dosage alone makes it so,” a foundational idea in dose-response thinking.
2.2 The Receptor Concept
The turning point came in the late 19th and early 20th centuries. John Newport Langley (1852–1925) studied the effects of pilocarpine and atropine on salivary secretion and proposed the existence of a “receptive substance” in cells that drugs interact with. Paul Ehrlich (1854–1915), working on chemotherapy and dyes, coined the phrase “Corpora non agunt nisi fixata” (substances do not act unless bound), cementing the idea that drugs must bind to specific cellular components to exert an effect.
2.3 Quantitative Pharmacodynamics and the Molecular Biology Era
In the 1920s and 1930s, Alfred J. Clark and others pioneered the application of mathematical models to drug-receptor interactions. Clark’s work on occupancy theory—that the effect of a drug is proportional to the number of receptors occupied—laid the groundwork for modern dose-response analysis. The latter half of the 20th century saw the identification and cloning of receptors, the discovery of G-protein-coupled receptors, ion channels, and nuclear receptors. The concepts of “spare receptors,” biased agonism, and allosteric modulation expanded pharmacodynamics far beyond a simple lock-and-key model. Today, pharmacodynamics integrates molecular biology, structural biology, genetics, and computational modeling to design drugs with ever-greater precision.
3. Core Principles of Pharmacodynamics
Before diving into specific mechanisms, it helps to understand several foundational principles that underpin all pharmacodynamic reasoning:
- Drugs Do Not Create New Functions; They Modulate Existing Ones: A drug typically mimics or blocks endogenous substances (neurotransmitters, hormones, etc.) or alters the rate of ongoing physiological processes. For example, a beta-blocker doesn’t invent a new cardiac function; it simply prevents adrenaline from binding to its receptor, thereby slowing the heart.
- Affinity and Intrinsic Activity (Efficacy): A drug’s ability to bind to its receptor is called affinity. Once bound, the drug’s ability to activate the receptor and produce a cellular response is called intrinsic activity or efficacy. A drug can have high affinity but zero efficacy (a pure antagonist) or high affinity and high efficacy (a full agonist).
- The Lock-and-Key (and Induced-Fit) Model: The classical analogy is that the drug (key) fits into a receptor (lock). Modern understanding incorporates the induced-fit model, where the receptor changes shape upon binding, leading to activation or inhibition.
- Receptor Occupancy and Response: Historically, the relationship between the fraction of receptors occupied and the magnitude of response was thought to be linear, but we now know that signal amplification and spare receptors often make the response curve steeper.
- Selectivity and Side Effects: No drug is perfectly selective for a single receptor subtype. At higher concentrations, a drug may bind to related receptors, producing side effects.
4. Mechanism of Action of Drugs: How Medicines Work
The phrase mechanism of action of drugs (MoA) is one of the most searched and clinically important keywords in pharmacodynamics. It refers to the specific biochemical interaction through which a drug substance produces its pharmacological effect. MoA can be classified broadly into receptor-mediated mechanisms and non-receptor-mediated mechanisms.
4.1 Receptor-Mediated Mechanisms
Most drugs exert their effects by interacting with specific macromolecular components of the cell, called receptors. Receptors are typically proteins that can be grouped into several families:
- Ligand-Gated Ion Channels (Ionotropic Receptors): These are membrane-spanning proteins that form a pore which opens in response to neurotransmitter binding, allowing ions to flow across the membrane. Examples include the nicotinic acetylcholine receptor, GABA_A receptor, and NMDA glutamate receptor. Benzodiazepines bind to an allosteric site on the GABA_A receptor and enhance the channel’s opening frequency, increasing chloride ion influx and producing sedation.
- G-Protein-Coupled Receptors (GPCRs): The largest receptor family, GPCRs consist of a single polypeptide chain that weaves through the cell membrane seven times (7TM receptors). Upon ligand binding, the receptor activates an intracellular G-protein, which in turn modulates various effector systems (adenylyl cyclase, phospholipase C, ion channels). Examples: beta-adrenoceptors (targeted by beta-blockers), histamine H2 receptors (targeted by ranitidine), opioid receptors (targeted by morphine).
- Enzyme-Linked Receptors (Kinase-Linked Receptors): These receptors have an extracellular ligand-binding domain and an intracellular domain that possesses enzymatic (usually tyrosine kinase) activity. Insulin, growth factors, and many cytokines act through such receptors. The binding of insulin to its receptor triggers autophosphorylation, initiating a cascade that leads to glucose transporter translocation.
- Nuclear (Intracellular) Receptors: These are soluble receptors located inside the cell, often in the cytoplasm or nucleus, that bind lipophilic ligands capable of crossing the plasma membrane. Steroid hormones, thyroid hormones, vitamin D, and retinoic acid all act via nuclear receptors. Glucocorticoids like prednisone work this way, modifying the expression of inflammatory proteins—a slower onset but long-lasting effect.
4.2 Non-Receptor Mediated Mechanisms
Not all drugs require a specific receptor. Some work through:
- Enzyme Inhibition: NSAIDs inhibit cyclooxygenase (COX) enzymes, reducing prostaglandin synthesis; ACE inhibitors block angiotensin-converting enzyme, lowering blood pressure.
- Ion Channel Modulation: Local anesthetics like lidocaine block voltage-gated sodium channels, preventing nerve impulse propagation.
- Transport Protein Interaction: Antidepressants (SSRIs) block the serotonin reuptake transporter; diuretics like furosemide inhibit the Na-K-2Cl cotransporter in the kidney.
- Physicochemical Mechanisms: Antacids neutralize stomach acid without involving a receptor; osmotic diuretics like mannitol increase urine output by altering osmotic gradients.
- Nucleic Acid Interaction: Chemotherapeutic agents can intercalate into DNA or cross-link strands, impairing replication. Alkylating agents like cyclophosphamide are classic examples.
- Antibody-Based Therapies: Monoclonal antibodies bind to specific proteins (e.g., TNF-alpha inhibitors in rheumatoid arthritis), neutralizing them or marking cells for immune destruction.
5. Drug Receptors and Drug Action: Agonists, Antagonists, and Beyond
The phrase drug receptors and drug action encapsulates the core interactions that determine whether a drug will activate or block a pathway. To fully appreciate pharmacodynamics, one must master the spectrum of drug-receptor interactions.
5.1 Agonists
An agonist is a drug that binds to a receptor and activates it, producing a biological response. Agonists can be classified into:
- Full Agonists: Produce the maximum tissue response possible when binding to a receptor (high intrinsic activity). Even when they occupy fewer than 100% of receptors (due to spare receptors), they can elicit a maximal effect. Example: Morphine at mu-opioid receptors.
- Partial Agonists: Bind and activate the receptor but produce only a submaximal response even at full receptor occupancy. They possess intermediate intrinsic activity. Because they occupy receptors, partial agonists can act as functional antagonists in the presence of a full agonist by competing for binding sites. Example: Buprenorphine at mu-opioid receptors—it provides pain relief but with a ceiling effect on respiratory depression, making it safer.
- Inverse Agonists: In systems with constitutive (basal) receptor activity, an inverse agonist binds to the receptor and reduces its activity below the basal level. This concept is crucial for receptors that are active even in the absence of a ligand. Example: Some antihistamines are inverse agonists at the H1 receptor, reducing its constitutive signaling.
5.2 Antagonists
Antagonists bind to receptors but do not activate them; they block the action of agonists. They have zero intrinsic activity.
- Competitive Antagonists (Reversible): Bind reversibly to the same site as the agonist. They can be overcome by increasing the agonist concentration. On a dose-response curve, competitive antagonism shifts the agonist curve to the right (increased EC50) without reducing the maximal effect if agonist dose is raised sufficiently. Example: Naloxone at opioid receptors—it reverses opioid overdose by displacing the agonist.
- Irreversible Antagonists: Bind covalently or with very high affinity to the receptor site, permanently inactivating the receptor. Increasing agonist concentration cannot surmount the blockade, leading to a reduction in maximal response. Example: Phenoxybenzamine, an irreversible alpha-adrenoceptor antagonist used in pheochromocytoma.
- Non-Competitive Antagonists: Bind to a different site (allosteric) on the receptor or to a downstream signaling component, preventing the agonist from producing an effect regardless of concentration. They also depress the maximal response. Example: Ketamine blocks NMDA receptor channels in a use-dependent manner distinct from the glutamate binding site.
5.3 Allosteric Modulators and Biased Agonism
Allosteric modulators bind to a site distinct from the orthosteric (primary) ligand-binding site and either enhance (positive allosteric modulator, PAM) or inhibit (negative allosteric modulator, NAM) receptor activation. Unlike orthosteric drugs, they tend to have a ceiling effect and greater receptor subtype selectivity. Example: Benzodiazepines are PAMs at GABA_A receptors. Biased agonism (functional selectivity) is a fascinating advancement where some ligands stabilize specific receptor conformations that preferentially activate one downstream signaling pathway over another. A beta-blocker like carvedilol, for instance, blocks G-protein-mediated contractile effects but can activate beta-arrestin-mediated pathways that promote cardioprotective signaling.
5.4 Receptor Regulation
Drug receptors are not static. Chronic agonist exposure can lead to desensitization (reduced responsiveness) and downregulation (decreased receptor number). Conversely, prolonged antagonist exposure can cause supersensitivity and upregulation. These phenomena explain drug tolerance, withdrawal symptoms, and rebound effects. For example, sudden withdrawal of long-term beta-blocker therapy can lead to rebound tachycardia due to receptor upregulation.
6. Dose-Response Relationships: Quantifying Drug Action
The dose-response relationship is a fundamental quantitative tool in pharmacodynamics. It describes how the effect of a drug changes with increasing dose or concentration. There are two main types: graded and quantal.
6.1 Graded Dose-Response Curves
These curves plot the magnitude of response (e.g., change in blood pressure, muscle contraction force) against increasing drug concentration in a single system or individual. The typical curve is sigmoidal when plotted as effect versus log concentration. Key parameters derived from the graded curve:
- Emax (Maximal Efficacy): The maximum effect a drug can produce. A full agonist reaches the tissue’s maximal capability, while a partial agonist has a lower Emax.
- EC50 (Half-Maximal Effective Concentration): The concentration at which the drug produces 50% of its maximal effect. It is a measure of potency—lower EC50 means higher potency.
- Potency vs. Efficacy: Potency refers to the amount of drug needed to produce an effect (often related to affinity and receptor density), while efficacy refers to the maximal effect a drug can produce regardless of dose. Clinically, efficacy is usually more important than potency.
6.2 Quantal Dose-Response Curves
Quantal curves represent the percentage of a population that responds to a given dose with an all-or-none effect (e.g., pain relief, death in toxicity studies). They are vital for determining:
- ED50 (Median Effective Dose): Dose at which 50% of the population exhibits the desired therapeutic effect.
- TD50 (Median Toxic Dose): Dose at which 50% experiences a particular toxic effect.
- LD50 (Median Lethal Dose): Dose at which 50% of animals die (in preclinical studies).
6.3 Therapeutic Index and Therapeutic Window
The Therapeutic Index (TI) is the ratio TD50 / ED50 (or in animal studies, LD50 / ED50). A higher TI indicates a wider safety margin. However, the more clinically useful concept is the therapeutic window, the range of drug concentrations that provides efficacy without unacceptable toxicity. Drugs with a narrow therapeutic window (e.g., warfarin, digoxin, lithium) require therapeutic drug monitoring to keep levels within the safe range. A steep dose-response curve implies that a small change in dose can produce a large change in effect, which may be clinically risky if the drug’s therapeutic window is narrow.
7. Clinical Applications of Pharmacodynamics
Pharmacodynamics is not just an academic exercise; it directly impacts patient care in countless ways.
- Personalized Dosing: By understanding receptor polymorphisms, a clinician might select a different beta-agonist for an asthmatic whose beta-2 receptor genotype renders them less responsive to albuterol.
- Managing Drug Interactions: If two drugs act on the same receptor (e.g., an anticholinergic and a cholinergic agonist), PD antagonism will occur. Knowing this, clinicians avoid combining drugs with opposing effects or use them strategically.
- Tachyphylaxis and Tolerance: Repeated use of nitrates leads to tolerance through depletion of sulfhydryl groups and reduced cGMP response—a PD tolerance. A nitrate-free interval is prescribed to restore efficacy.
- Drug Switching: When a patient doesn’t respond to one class of antihypertensive, understanding the MoA guides the switch: for example, moving from an ACE inhibitor to an angiotensin receptor blocker may be based on PD considerations regarding bradykinin-mediated cough.
- Antidote Use: Naloxone for opioid overdose is a direct application of competitive antagonism at mu receptors.
- Cancer Therapy: Targeted agents like imatinib (a tyrosine kinase inhibitor) bind to the BCR-ABL fusion protein in chronic myeloid leukemia. PD monitoring of target inhibition (phosphorylation levels) helps assess treatment response.
8. Pharmacodynamics in Drug Development
8.1 Target Identification and Validation
The drug development process begins with identifying and confirming disease-associated biological targets—typically receptors, enzymes, or ion channels. Pharmacodynamic studies validate that modulating the target produces the desired therapeutic effect.
8.2 Lead Optimization and Preclinical PD
Once a lead compound is identified, pharmacodynamic assays measure its potency, efficacy, and selectivity at the target. Preclinical PD studies in animal models establish the dose-response relationship and predict the human dose range. PK/PD modeling integrates pharmacokinetic and pharmacodynamic data to design optimal dosing regimens for clinical trials.
8.3 Clinical Pharmacodynamics
In Phase I and II clinical trials, pharmacodynamic biomarkers (e.g., receptor occupancy, enzyme inhibition, changes in physiological parameters) demonstrate proof of mechanism and proof of concept. These PD endpoints guide dose selection for pivotal Phase III trials.
9. Factors Affecting Pharmacodynamics
| Factor | Effect on Pharmacodynamics |
|---|---|
| Age | Neonates and elderly patients often have altered receptor sensitivity and homeostatic mechanisms. |
| Genetics | Receptor polymorphisms and signaling protein variants can alter drug response (pharmacogenetics). |
| Disease States | Diseases can upregulate or downregulate receptors; hepatic or renal impairment alters drug concentrations at the target. |
| Drug Interactions | Pharmacodynamic interactions occur when two drugs act on the same or related pathways (additive, synergistic, or antagonistic effects). |
| Tolerance | Repeated drug exposure can lead to receptor desensitization, downregulation, or depletion of mediators. |
| Circadian Rhythms | Receptor expression and hormonal axes show diurnal variation, affecting drug response (chronopharmacology). |
Q1: What is pharmacodynamics? | فارماکوڈائنامکس کیا ہے؟
Q2: What is the difference between pharmacodynamics and pharmacokinetics?
Q3: What is the mechanism of action of drugs?
Q4: What are drug receptors and how do they relate to drug action?
Q5: What is the difference between an agonist and an antagonist?
Q6: What is the difference between potency and efficacy?
Q7: What is a dose-response curve?
Q8: What is the therapeutic index?
Q9: What are spare receptors?
Q10: How does tolerance develop from a pharmacodynamic perspective?
Q11: What is biased agonism (functional selectivity)?
Q12: What is the difference between competitive and non-competitive antagonism?
Q13: How do nuclear receptors work?
Q14: Can a drug have more than one mechanism of action?
Q15: Are all drug actions receptor-mediated?
Q16: What is pharmacodynamic drug interaction?
Q17: What is the therapeutic window?
Q18: How do allosteric modulators differ from orthosteric drugs?
Q19: What is receptor desensitization and downregulation?
Q20: Why is understanding pharmacodynamics important for clinicians?
Pharmacodynamics is the heartbeat of modern pharmacology—a field that transforms molecules into medicines and biological insights into life-saving therapies. From the ancient wisdom of dosage to the cutting-edge design of biased agonists, our understanding of how drugs work continues to evolve, driven by molecular biology and computational science.
We have journeyed through the mechanism of action of drugs, dissected the role of drug receptors and drug action, distinguished between agonists, antagonists, and modulators, and clarified the ever-important contrast of pharmacodynamics vs pharmacokinetics. We also addressed the Urdu question فارماکوڈائنامکس کیا ہے؟ to ensure that language is no barrier to understanding this critical science.
Ultimately, pharmacodynamics empowers clinicians to prescribe rationally, helps researchers innovate safely, and gives patients confidence that their medications are not mysterious potions but precisely engineered tools interacting with the body’s innate machinery. The next time you take a pill, you can appreciate the elegant dance between drug and receptor—an invisible but beautifully orchestrated event governed by the principles laid out in this article.
As with all medical sciences, this knowledge is intended to inform and educate. No article can replace the personalized judgment of a healthcare provider who weighs your unique physiology, genetics, and circumstances against the pharmacodynamic profile of a drug. That collaboration—between patient, provider, and the science of pharmacodynamics—is where true healing begins.
11. References and Suggested Readings
1. Rang HP, Ritter JM, Flower RJ, Henderson G. Rang & Dale’s Pharmacology. 9th ed. Elsevier; 2020.
2. Brunton LL, Hilal-Dandan R, Knollmann BC, eds. Goodman & Gilman’s: The Pharmacological Basis of Therapeutics. 13th ed. McGraw-Hill; 2018.
3. Katzung BG, Vanderah TW. Basic & Clinical Pharmacology. 15th ed. McGraw-Hill; 2021.
4. Kenakin T. Pharmacology in Drug Discovery and Development: Understanding Drug Response. 2nd ed. Academic Press; 2017.
5. Neubig RR, Spedding M, Kenakin T, Christopoulos A. International Union of Pharmacology Committee on Receptor Nomenclature and Drug Classification. XXXVIII. Update on terms and symbols in quantitative pharmacology. Pharmacol Rev. 2003;55(4):597-606.
6. Holford NHG, Sheiner LB. Understanding the dose-effect relationship: clinical application of pharmacokinetic-pharmacodynamic models. Clin Pharmacokinet. 1981;6(6):429-453.
7. Ross EM, Kenakin TP. Pharmacodynamics: mechanisms of drug action and the relationship between drug concentration and effect. In: Hardman JG, Limbird LE, eds. Goodman & Gilman’s The Pharmacological Basis of Therapeutics. 10th ed. McGraw-Hill; 2001:31-44.
8. Rowland M, Tozer TN. Clinical Pharmacokinetics and Pharmacodynamics: Concepts and Applications. 4th ed. Lippincott Williams & Wilkins; 2011.
9. Meibohm B, Derendorf H. Basic concepts of pharmacokinetic/pharmacodynamic (PK/PD) modelling. Int J Clin Pharmacol Ther. 1997;35(10):401-13.
10. Mangoni AA, Jackson SHD. Age-related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications. Br J Clin Pharmacol. 2004;57(1):6-14.
Last Updated: June 2026 | Version: 1.0 | Review Frequency: Annual review recommended
This article has been written with a focus on evidence-based medicine, clinical pharmacodynamics, and practical application for medical students, residents, and practicing clinicians. The content aligns with contemporary pharmacological principles and integrates the latest concepts in receptor theory, biased agonism, and PK/PD modeling.