Pharmacology Basics What is Pharmacology Complete Guide for Medical Students and Healthcare Professionals
Pharmacology Basics? A Comprehensive Guide for Medical Students and Healthcare Professionals | فارماکولوجی کیا ہے؟

Pharmacology is the bedrock of modern medicine, bridging the gap between basic science and clinical practice. For medical students and healthcare professionals, a deep understanding of pharmacology is not merely about memorizing drug names—it is about grasping the fundamental principles that govern how drugs interact with the human body, how the body processes these agents, and how to apply this knowledge to optimize patient care. This comprehensive guide provides a research-based foundation in pharmacology, from its historical origins to the latest concepts in pharmacokinetics, pharmacodynamics, and personalized medicine.
1. Introduction: The Science of Healing
1.1 Defining Pharmacology
Pharmacology is the branch of medicine and biology concerned with the study of drugs and their effects on living organisms. The term derives from the Greek word pharmakon (drug or medicine) and logia (study), reflecting its core mission: the scientific investigation of medicinal substances. As an integrated medical science, pharmacology draws upon principles from chemistry, physiology, biochemistry, and molecular biology to provide a comprehensive understanding of drug action and usage. Unlike nutrients, which add new physiological functions, drugs typically do not introduce new functions but rather alter the rates of existing biological processes.
Pharmacology can be broadly divided into two main areas:
- Pharmacodynamics: The study of how drugs affect the body—examining the relationship between drug concentration and effect, including mechanisms of action, therapeutic effects, and side effects.
- Pharmacokinetics: The study of how the body absorbs, distributes, metabolizes, and excretes drugs—often summarized by the acronym ADME.
1.2 Pharmacology vs. Pharmacy: Understanding the Distinction
It is essential to distinguish pharmacology from pharmacy, as these terms are often confused:
- Pharmacology is the science of drugs—their properties, effects, and mechanisms of action. It is a basic and clinical science that seeks to understand how drugs work.
- Pharmacy is the practice of preparing, compounding, and dispensing drugs. It includes the collection, isolation, purification, synthesis, and standardization of medicinal substances.
While pharmacologists study drug actions and develop new therapies, pharmacists ensure that medications are prepared correctly and used safely. Both disciplines are essential to patient care, but they represent different facets of the medication use process.
2. History of Pharmacology: From Ancient Remedies to Modern Science
2.1 Ancient Foundations
The origins of pharmacology trace back to ancient civilizations, where herbal remedies and natural substances were used to treat ailments. The Greek physician Hippocrates (circa 460–370 BCE) laid the foundation for scientific medicine, emphasizing observation and rational treatment. A landmark contribution came from Dioscorides, a Greek physician who wrote De Materia Medica in the 1st century CE. This five-volume work systematically documented approximately 600 medicinal plants and their uses, serving as the authoritative pharmacological reference for over 1,500 years.
2.2 The Birth of Modern Pharmacology
The transition from empirical observation to experimental science began in the 19th century. Several key developments marked this transformation:
- Isolation of Active Compounds: By the early 19th century, French and German chemists had isolated many active substances from their crude plant sources—including morphine, strychnine, atropine, and quinine. This enabled the standardization and purification of drugs, moving beyond crude plant preparations.
- Foundational Experiments: In 1809, François Magendie demonstrated that the convulsant action of nux vomica (containing strychnine) originated in the spinal cord. In 1842, Claude Bernard discovered that the arrow poison curare acts at the neuromuscular junction, interrupting nerve-to-muscle signaling.
- Establishment as a Discipline: Pharmacology emerged as a distinct scientific discipline when the first university chair was established in 1847, when Rudolf Buchheim was appointed professor of pharmacology at the University of Dorpat in Estonia.
- The Founder of Modern Pharmacology: Oswald Schmiedeberg (1838–1921) is generally recognized as the founder of modern pharmacology. He published a classic textbook, Outline of Pharmacology (1878), helped found the first pharmacological journal, and established a school at Strasbourg that became the nucleus from which independent pharmacology departments were established worldwide.
2.3 The 20th Century and Beyond
The 20th century witnessed an explosion of pharmacological discovery. The development of antibiotics (such as penicillin), hormonal drugs (insulin and cortisone), and countless other therapeutic agents revolutionized medicine. Pharmacologists became increasingly aware of the relationship between chemical structure and biological effect, leading to the systematic study of structure-activity relationships. Today, pharmacology continues to evolve with advances in molecular biology, genomics, and personalized medicine, seeking more effective and safer therapeutic agents.
3. Importance of Pharmacology
Pharmacology is fundamental to modern healthcare for several compelling reasons:
- Rational Therapeutics: Pharmacology provides the scientific basis for rational drug therapy. Understanding how drugs work, how they are processed by the body, and how they interact with other medications enables clinicians to select the most appropriate treatment for each patient.
- Patient Safety: Knowledge of pharmacokinetics, pharmacodynamics, and adverse drug reactions is essential for preventing medication errors and minimizing harm. Adverse drug reactions are a major cause of emergency department visits and hospitalizations, with studies estimating that 10–30% of these visits are drug-related.
- Drug Development: Pharmacology is the cornerstone of the drug discovery process. Pharmacologists screen for desired activity, determine mechanisms of action, and quantify drug activity.
- Personalized Medicine: Advances in pharmacogenetics and pharmacogenomics are enabling personalized approaches to drug therapy, tailoring treatments based on individual genetic profiles to maximize efficacy and minimize toxicity.
- Public Health: Pharmacology contributes to public health through pharmacovigilance—the monitoring of drug safety in the general population—and through the development of vaccines, antimicrobials, and other agents that combat infectious diseases.
4. Branches of Pharmacology
Pharmacology encompasses numerous specialized branches, each focusing on different aspects of drug action and application:
| Branch | Description |
|---|---|
| Pharmacokinetics | Study of drug absorption, distribution, metabolism, and excretion (ADME). |
| Pharmacodynamics | Study of drug mechanisms of action and the relationship between drug concentration and effect. |
| Therapeutics | Art and science of disease treatment—applying pharmacological knowledge to prevent and cure disease. |
| Chemotherapy | Treatment of diseases by chemicals that kill cells, particularly microorganisms and neoplastic cells. |
| Toxicology | Study of poisons and poisoning—the adverse effects of chemicals on living organisms. |
| Clinical Pharmacology | Identifies and assesses the therapeutic effectiveness and safety of drugs in humans. |
| Pharmacognosy | Study of the botanical sources of drugs—the identification and characterization of medicinal substances derived from natural sources. |
| Pharmacogenetics | Study of genetic variations that influence drug response, enabling personalized medicine approaches. |
| Pharmacoepidemiology | Study of drug use and effects in large populations, including the identification of adverse drug reactions and patterns of medication use. |
| Pharmacoeconomics | Evaluation of the economic aspects of drug therapy, including cost-effectiveness analysis and resource allocation. |
5. Drug Classification
Drugs can be classified in multiple ways, each serving different purposes in clinical practice and education:
5.1 By Therapeutic Use
This classification groups drugs according to the condition they treat:
- Antihypertensives: Lower blood pressure
- Antibiotics: Treat bacterial infections
- Antidepressants: Treat depression
- Anticoagulants: Prevent blood clotting
- Antidiabetics: Control blood glucose
5.2 By Mechanism of Action
This classification groups drugs based on how they produce their effects:
- Receptor agonists: Activate receptors to produce a response
- Receptor antagonists: Block receptors to prevent a response
- Enzyme inhibitors: Block enzyme activity
- Ion channel modulators: Alter ion flux across cell membranes
5.3 By Chemical Structure
Drugs with similar chemical structures often share similar properties and mechanisms of action. Examples include:
- Beta-lactam antibiotics (penicillins, cephalosporins)
- Benzodiazepines (diazepam, lorazepam)
- Opioids (morphine, fentanyl)
5.4 By Source
Drugs can be derived from various sources:
- Plants: Digitalis, morphine, quinine
- Animals: Insulin, heparin
- Microorganisms: Penicillin, streptomycin
- Minerals: Lithium, magnesium
- Synthetic: Most modern pharmaceuticals
- Semi-synthetic: Chemically modified natural products
6. Drug Names
Every drug has multiple names, and understanding this nomenclature is essential for patient safety:
- Chemical Name: Describes the molecular structure of the drug using standard chemical nomenclature. For example, the chemical name for acetaminophen is N-acetyl-p-aminophenol.
- Generic Name (Non-proprietary Name): The official name assigned by national or international authorities (such as the USAN or WHO INN). Examples include acetaminophen, amoxicillin, and metformin.
- Brand Name (Proprietary Name): Assigned by the manufacturer and protected by trademark. Examples include Tylenol® (acetaminophen), Amoxil® (amoxicillin), and Glucophage® (metformin).
Confusion between drug names is a common cause of medication errors. Healthcare professionals must be fluent in both generic and brand names.
7. Dosage Forms
Dosage forms are the physical forms in which drugs are manufactured and administered:
| Type | Examples |
|---|---|
| Liquid | Solutions, suspensions, syrups, elixirs, tinctures, emulsions |
| Solid | Tablets, capsules, powders, granules, suppositories, implants |
| Semi-solid | Ointments, creams, gels, pastes |
| Other | Transdermal patches, inhalation aerosols, injectable solutions |
The choice of dosage form depends on factors including the drug’s properties, the desired route of administration, and patient-specific considerations.
8. Routes of Drug Administration
The route of administration significantly influences drug absorption, onset of action, and therapeutic effect:
8.1 Enteral Routes
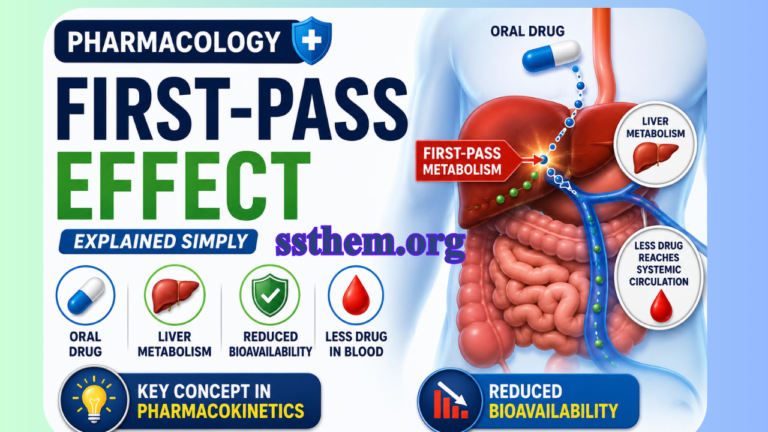
- Oral: Most convenient, safest, and least expensive. Subject to first-pass metabolism.
- Sublingual and Buccal: Rapid absorption through oral mucosa, bypassing first-pass metabolism.
- Rectal: Useful when oral administration is not possible.
8.2 Parenteral Routes
- Intravenous (IV): Rapid onset, precise control over drug levels.
- Intramuscular (IM): Moderate absorption rates.
- Subcutaneous (SC): Injection beneath the skin.
- Intrathecal: Injection into the space around the spinal cord.
8.3 Topical Routes
- Cutaneous: Applied to the skin for local or systemic effects.
- Transdermal: Delivered through the skin via patches.
- Ocular, Otic, Nasal, Inhalation: For local or systemic effects.
9. Drug Development Process
The journey from laboratory discovery to clinical use is a long and complex process, typically taking 10 to 15 years:
9.1 Target Identification and Validation
The process begins with identifying and confirming disease-associated biological targets.
9.2 Hit and Lead Discovery
Compounds that interact with the target are identified and optimized for potency and selectivity.
9.3 Preclinical Phase
In vitro and in vivo studies assess the compound’s safety, efficacy, pharmacokinetics, and pharmacodynamics.
9.4 Clinical Trials
If preclinical studies are successful, the drug enters clinical trials, conducted in phases:
- Phase I: Trials in a small number of healthy volunteers to assess safety and dosage.
- Phase II: Trials in a small number of subjects with the disease to assess efficacy and side effects.
- Phase III: Trials in a large number of subjects with the disease to confirm efficacy and monitor adverse reactions.
9.5 Regulatory Review and Approval
Data from clinical trials are submitted to regulatory authorities (such as the FDA or EMA) for review and approval.
9.6 Post-Marketing Surveillance (Phase IV)
Continuous monitoring of the drug’s long-term safety and effectiveness in the broader population.
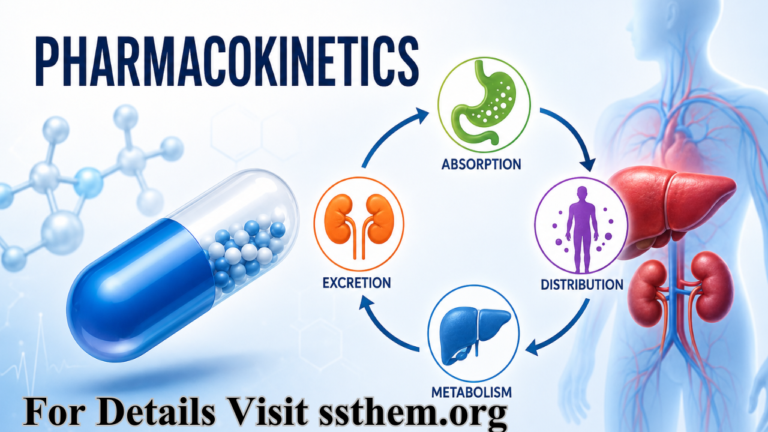
10. Pharmacokinetics (ADME)
Pharmacokinetics describes what the body does to a drug—the processes of absorption, distribution, metabolism, and excretion.
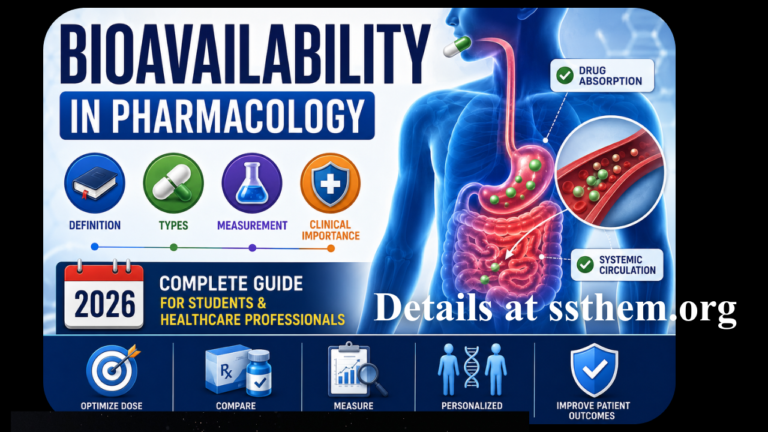
10.1 Absorption
Absorption is the process by which drugs enter the body and travel from the site of administration into the body’s circulation. Factors affecting absorption include:
- Route of administration
- Drug formulation
- Physicochemical properties of the drug (solubility, molecular size)
- Blood flow to the absorption site
- Presence of food or other drugs
10.2 Distribution
Distribution is the process by which medication is spread throughout the body. Key factors include:
- Blood flow to tissues
- Drug binding to plasma proteins
- Drug lipophilicity (ability to cross cell membranes)
- Tissue barriers (e.g., blood-brain barrier, placental barrier)
Volume of Distribution (Vd): A theoretical volume that relates the amount of drug in the body to the concentration in plasma. A large Vd indicates extensive tissue distribution.
10.3 Metabolism
Metabolism (biotransformation) involves the enzymatic conversion of drugs into metabolites. The liver is the primary site of drug metabolism, though other organs also contribute.
- Phase I Reactions: Functionalization reactions (oxidation, reduction, hydrolysis) that introduce or expose functional groups.
- Phase II Reactions: Conjugation reactions that attach polar molecules to the drug or its Phase I metabolite, increasing water solubility and facilitating excretion.
- First-Pass Effect: Metabolism of a drug before it reaches systemic circulation, reducing bioavailability. This occurs primarily with orally administered drugs.
10.4 Excretion
Excretion is the process by which the body eliminates drugs and their metabolites. The kidneys are the primary route of excretion, though drugs may also be excreted through:
- Bile
- Lungs
- Sweat
- Saliva
- Breast milk
Half-Life (t½): The time required for the plasma concentration of a drug to decrease by 50%. Half-life determines dosing frequency and time to steady-state. Complete Details of Half-Life Here
Clearance: The volume of plasma from which a drug is completely removed per unit time.
11. Pharmacodynamics
Pharmacodynamics describes what the drug does to the body—the mechanisms of drug action and the relationship between drug concentration and effect.
11.1 Mechanisms of Drug Action
Drugs produce their effects through various mechanisms:
- Receptor Interactions: Many drugs act by binding to receptors—specialized proteins on cell surfaces or within cells that mediate physiological responses.
- Enzyme Interactions: Drugs may inhibit or activate enzymes, altering biochemical pathways.
- Ion Channel Modulation: Drugs may open or close ion channels, affecting cellular excitability.
- Transport Systems: Drugs may interfere with or utilize transport proteins.
- Physicochemical Interactions: Some drugs act through non-specific physicochemical mechanisms (e.g., antacids neutralizing stomach acid).
11.2 Drug Receptors
Receptors are the molecular targets through which drugs produce their effects. Most receptors are proteins that recognize and respond to endogenous signaling molecules (neurotransmitters, hormones).
Types of Receptors:
- Ligand-gated ion channels (ionotropic receptors): Fast synaptic transmission
- G-protein coupled receptors (GPCRs): The largest receptor family, mediating responses to numerous hormones and neurotransmitters
- Enzyme-linked receptors: Receptors with intrinsic enzymatic activity (e.g., receptor tyrosine kinases)
- Intracellular receptors: Receptors located inside cells that bind lipophilic ligands (e.g., steroid hormone receptors)
11.3 Drug-Receptor Interactions
- Agonists: Drugs that bind to receptors and activate them, producing a response. Full agonists produce maximal response; partial agonists produce submaximal response even at full receptor occupancy.
- Antagonists: Drugs that bind to receptors but do not activate them, blocking the action of agonists. Antagonists may be competitive (reversible) or non-competitive (irreversible).
- Affinity: The strength of binding between a drug and its receptor.
- Efficacy: The ability of a drug to produce a response once bound to its receptor.
- Potency: The amount of drug required to produce a given effect (related to affinity and efficacy).
11.4 Dose-Response Relationships
- Graded Dose-Response Curves: Plot the effect of increasing drug concentrations on a continuous scale. Key parameters include EC50 (the concentration producing 50% of the maximal effect) and Emax (the maximal effect achievable).
- Quantal Dose-Response Curves: Plot the proportion of a population that responds to a given dose. Key parameters include ED50 (the dose producing a response in 50% of the population) and LD50 (the dose lethal to 50% of the population in animal studies).
12. Therapeutic Index
The therapeutic index (TI) is a measure of drug safety that compares the dose required to produce a therapeutic effect to the dose that produces toxicity.
12.1 Calculation
TI = LD50 / ED50
Where:
- LD50 = median lethal dose (dose lethal to 50% of animals)
- ED50 = median effective dose (dose producing therapeutic effect in 50% of patients)
12.2 Clinical Interpretation
- High Therapeutic Index: A wide margin of safety (e.g., penicillin, TI > 100)
- Low Therapeutic Index: A narrow margin of safety requiring careful monitoring (e.g., digoxin, lithium, warfarin)
12.3 Therapeutic Window
The therapeutic window is the range of drug concentrations between the minimum effective concentration and the minimum toxic concentration. Drugs with a narrow therapeutic window require therapeutic drug monitoring to maintain concentrations within this range.
12.4 Margin of Safety
Some authorities prefer the margin of safety (or safety margin), which compares the dose that is lethal to 1% of the population (LD1) to the dose that is effective in 99% (ED99), providing a more conservative estimate of safety.
13. Adverse Drug Reactions
Adverse Drug Reactions (ADRs) are responses to a medicinal product that are noxious and unintended.
13.1 Classification (Rawlins-Thompson)
| Type | Characteristics | Examples |
|---|---|---|
| Type A (Augmented) | Predictable, dose-dependent, related to pharmacological action | Hypoglycemia from insulin, bleeding from anticoagulants |
| Type B (Bizarre) | Unpredictable, not dose-dependent, related to individual susceptibility | Anaphylaxis to penicillin, idiosyncratic drug reactions |
| Type C (Chronic) | Related to prolonged drug use | Osteoporosis from corticosteroids, tardive dyskinesia |
| Type D (Delayed) | Occur after a delay, sometimes long after drug discontinuation | Carcinogenesis, teratogenesis |
| Type E (End-of-use) | Withdrawal reactions occurring upon drug discontinuation | Withdrawal syndrome from opioids or benzodiazepines |
13.2 Risk Factors for ADRs
- Age (very young and elderly)
- Polypharmacy (taking multiple medications)
- Renal or hepatic impairment
- Genetic factors
- Pregnancy
- Drug-drug interactions
14. Drug Interactions
Drug-drug interactions (DDIs) occur when one drug affects the action of another, potentially leading to increased toxicity or reduced efficacy.
14.1 Mechanisms of Drug Interactions
- Pharmacokinetic Interactions: One drug alters the ADME of another:
- Absorption: Changes in gastrointestinal motility, pH, or binding
- Distribution: Competition for plasma protein binding sites
- Metabolism: Enzyme induction (increasing metabolism) or inhibition (decreasing metabolism)
- Excretion: Competition for renal or biliary excretion pathways
- Pharmacodynamic Interactions: One drug alters the effect of another at the receptor or physiological level:
- Additive effects: Combined effect equals the sum of individual effects
- Synergistic effects: Combined effect exceeds the sum of individual effects
- Antagonistic effects: One drug reduces the effect of another
14.2 Clinically Significant Interactions
- Warfarin and many drugs: Increased bleeding risk
- Statins and CYP3A4 inhibitors: Increased risk of myopathy
- MAOIs and tyramine-containing foods: Hypertensive crisis
- Digoxin and many drugs: Altered digoxin levels
15. Clinical Applications
Pharmacology is the foundation of rational prescribing and patient care.
15.1 Evidence-Based Prescribing
Clinicians must integrate pharmacological knowledge with clinical evidence to select the most appropriate drug, dose, and regimen for each patient. This requires understanding:
- Drug efficacy and safety data from clinical trials
- Pharmacokinetic parameters that guide dosing
- Patient-specific factors that affect drug response
15.2 Therapeutic Drug Monitoring
For drugs with a narrow therapeutic window, therapeutic drug monitoring (TDM) ensures that drug concentrations remain within the therapeutic range while avoiding toxicity. Drugs commonly monitored include:
- Digoxin
- Lithium
- Aminoglycosides
- Vancomycin
- Antiepileptics (phenytoin, carbamazepine)
15.3 Individualizing Therapy
Pharmacology enables personalized approaches to therapy:
- Pharmacogenetics: Genetic testing to predict drug response or toxicity risk
- Renal and hepatic dosing: Adjusting doses based on organ function
- Age-based adjustments: Pediatric and geriatric dosing considerations
- Pregnancy and lactation: Understanding drug safety during these periods
16. Pharmacology in Different Medical Fields
Pharmacology is relevant to every medical specialty:
| Specialty | Key Pharmacological Considerations |
|---|---|
| Cardiology | Antihypertensives, antiarrhythmics, anticoagulants; managing drug interactions |
| Infectious Disease | Antimicrobial pharmacology; mechanisms of antibiotic resistance |
| Psychiatry | Psychopharmacology of antidepressants, antipsychotics, mood stabilizers |
| Oncology | Chemotherapy and targeted therapy; managing toxicity and drug resistance |
| Pediatrics | Age-specific pharmacokinetics and pharmacodynamics; weight-based dosing |
| Geriatrics | Age-related changes in pharmacokinetics; polypharmacy and drug interactions |
| Emergency Medicine | Rapid administration of life-saving drugs; managing overdoses and poisonings |
Q1: What is pharmacology?
Q2: What is the difference between pharmacology and pharmacy?
Q3: Who is considered the founder of modern pharmacology?
Q4: What are the two main branches of pharmacology?
Q5: What is a drug?
Q6: What does ADME stand for?
Q7: What is bioavailability?
Q8: What is first-pass metabolism?
Q9: What is half-life?
Q10: What is volume of distribution?
Q11: What is a receptor?
Q12: What is the difference between an agonist and an antagonist?
Q13: What is the therapeutic index?
Q14: What is potency?
Q15: What is efficacy?
Q16: What are adverse drug reactions?
Q17: What is a drug-drug interaction?
Q18: What is therapeutic drug monitoring?
Q19: What is pharmacogenetics?
Q20: What is the difference between Type A and Type B adverse drug reactions?
Q21: How long does drug development typically take?
Q22: What are the phases of clinical trials?
Q23: What is post-marketing surveillance?
Q24: How does aging affect pharmacokinetics?
Q25: Why is pharmacology important for medical students?
18. Conclusion
Pharmacology is the cornerstone of modern medicine. For medical students and healthcare professionals, mastering the principles of pharmacology is essential for providing safe, effective, and evidence-based patient care.
From the historical foundations laid by pioneers like Schmiedeberg to the cutting-edge advances in pharmacogenetics and personalized medicine, pharmacology continues to evolve as a discipline that bridges basic science and clinical practice. Understanding pharmacokinetics and pharmacodynamics enables clinicians to predict drug behavior, individualize therapy, and minimize adverse effects. Knowledge of drug development, drug interactions, and adverse reaction monitoring ensures that patients receive the benefits of pharmacotherapy while avoiding its harms.
As you continue your journey in medicine, remember that pharmacology is not merely a subject to be memorized for examinations—it is a practical, dynamic science that you will apply every day at the bedside. The drug you prescribe today is the result of decades of research, and your understanding of its pharmacology will determine whether it brings healing or harm.
Embrace pharmacology as a lifelong learning endeavor. Stay curious about new drugs, new mechanisms, and new evidence. And always remember: behind every drug is a patient whose well-being depends on your knowledge and judgment.
19. References and Suggested Readings
1. Brunton LL, Hilal-Dandan R, Knollmann BC, eds. Goodman & Gilman’s The Pharmacological Basis of Therapeutics. 13th ed. McGraw-Hill; 2018.
2. Katzung BG, Vanderah TW. Basic and Clinical Pharmacology. 15th ed. McGraw-Hill; 2021.
3. Rowland M, Tozer TN. Clinical Pharmacokinetics and Pharmacodynamics: Concepts and Applications. 4th ed. Lippincott Williams & Wilkins; 2011.
4. Birkett DJ. Pharmacokinetics Made Easy. 2nd ed. McGraw-Hill; 2010.
5. Buxton ILO, Benet LZ. Pharmacokinetics: The Dynamics of Drug Absorption, Distribution, Metabolism, and Elimination. In: Brunton LL, Hilal-Dandan R, Knollmann BC, eds. Goodman & Gilman’s The Pharmacological Basis of Therapeutics. 13th ed. McGraw-Hill; 2018.
6. Meibohm B, Derendorf H. Basic concepts of pharmacokinetic/pharmacodynamic (PK/PD) modelling. Int J Clin Pharmacol Ther. 1997;35(10):401-13.
7. Leucuta SE, Vlase L. Pharmacokinetics and metabolic drug interactions. Curr Clin Pharmacol. 2006;1(1):5-20.
8. Mangoni AA, Jackson SHD. Age‑related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications. Br J Clin Pharmacol. 2004;57(1):6-14.
9. Verbeeck RK, Musuamba FT. Pharmacokinetics and dosage adjustment in patients with renal dysfunction. Eur J Clin Pharmacol. 2009;65(8):757-73.
10. Westfall TC, Macarthur H, Westfall DP. Neurotransmission: The Autonomic and Somatic Motor Nervous Systems. In: Brunton LL, Hilal-Dandan R, Knollmann BC, eds. Goodman & Gilman’s The Pharmacological Basis of Therapeutics. 13th ed. McGraw-Hill; 2018.
11. US Food and Drug Administration. Guidance for Industry: Population Pharmacokinetics. 2022.
12. National Institute for Health and Care Excellence (NICE). Medicines optimisation: the safe and effective use of medicines to enable the best possible outcomes. NICE guideline NG5; 2015.
13. Winter ME. Basic Clinical Pharmacokinetics. 5th ed. Lippincott Williams & Wilkins; 2010.
14. Bauer LA. Applied Clinical Pharmacokinetics. 3rd ed. McGraw-Hill; 2014.
This educational resource is intended for medical students and healthcare professionals to enhance understanding of pharmacology. It is not a substitute for clinical judgment, individual patient assessment, or up‑to‑date prescribing information. Always consult current guidelines, local formularies, and a qualified healthcare provider before making therapeutic decisions.
Last Updated: June 2026 | Version: 2.0 | Review Frequency: Annual review recommended
This article has been written with a focus on evidence‑based medicine, clinical pharmacology, and practical application for medical students, residents, and practicing clinicians. The content aligns with contemporary pharmacological principles and antimicrobial stewardship practices.