Master ADME Pharmacokinetics in 4 Simple Steps: The Complete Guide to Drug Absorption, Distribution, Metabolism & Excretion
ADME Pharmacokinetics Explained: Drug Absorption, Distribution, Metabolism & Excretion in Pharmacology
A Comprehensive Evidence-Based Guide for Medical, Pharmacy & Dental Students
Pharmacokinetics is the cornerstone of rational drug therapy and clinical pharmacology. The ADME framework—Absorption, Distribution, Metabolism, and Excretion—describes the journey of a drug through the human body, determining its concentration at the site of action, duration of effect, and ultimate elimination. This comprehensive evidence-based guide examines each component of the ADME process in detail, addressing the fundamental clinical question: “How does the body process a drug from administration to elimination?” The answer depends on multiple factors: drug physicochemical properties, patient physiology, genetic variation, organ function, and drug-drug interactions. Drawing on current FDA guidance, clinical pharmacology principles, and contemporary research, this article provides medical, pharmacy, and dental students with a thorough understanding of pharmacokinetic principles essential for safe and effective prescribing.
1. Introduction to ADME Pharmacokinetics
 Pharmacokinetics, often described as “what the body does to a drug,” refers to the movement of drugs into, through, and out of the body—the time course of their absorption, bioavailability, distribution, metabolism, and excretion. Understanding these processes and their interplay, and employing pharmacokinetic principles, increases the probability of therapeutic success and reduces the occurrence of adverse drug events and drug-drug interactions.
Pharmacokinetics, often described as “what the body does to a drug,” refers to the movement of drugs into, through, and out of the body—the time course of their absorption, bioavailability, distribution, metabolism, and excretion. Understanding these processes and their interplay, and employing pharmacokinetic principles, increases the probability of therapeutic success and reduces the occurrence of adverse drug events and drug-drug interactions.
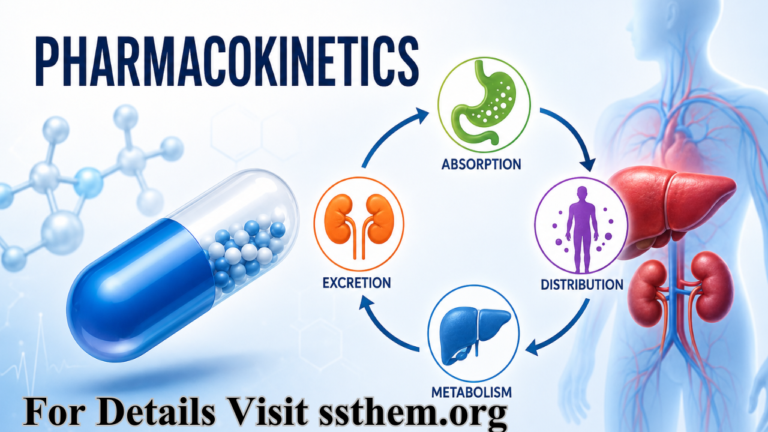
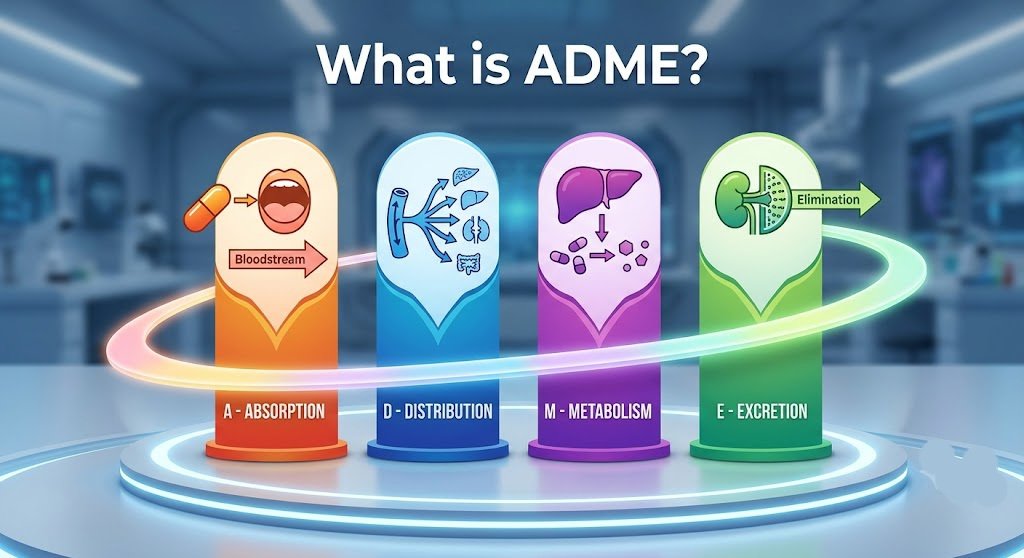
The acronym ADME represents the four fundamental processes that determine drug disposition:
- A – Absorption: Drug entry into the bloodstream from the site of administration
- D – Distribution: Movement of drug molecules throughout body tissues and organs
- M – Metabolism: Biochemical modification of the drug, primarily in the liver
- E – Excretion: Elimination of the drug and its metabolites from the body
The FDA emphasizes that clinical pharmacologists “own the dose”—helping determine the dosing regimen of a drug, including how much to give and how often to give it. This critical responsibility requires a deep understanding of ADME principles to optimize therapeutic outcomes while minimizing toxicity.
1.1 The Clinical Significance of Pharmacokinetics
Pharmacokinetics is essential in clinical medicine because it determines:
- Drug dosage and dosing intervals – How much and how often to administer
- Frequency of administration – Once daily, twice daily, or more frequent dosing
- Duration of action – How long the drug remains effective
- Toxicity risk – Potential for drug accumulation and adverse effects
- Therapeutic effectiveness – Achieving target concentrations at the site of action
- Individualized therapy – Adjusting doses for patient-specific factors
Key Insight: The FDA notes that important pharmacokinetic information communicated in drug labeling includes bioavailability, time to reach maximum concentration (Tmax), half-life (T1/2), major route of elimination, and percentage excreted in urine or feces. This information guides prescribing decisions and patient monitoring.
2. Drug Absorption
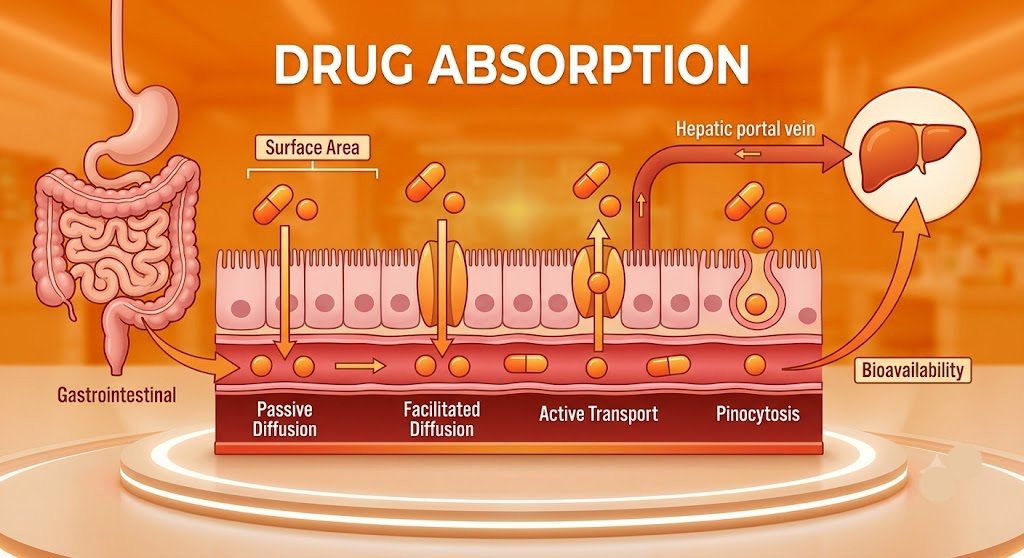 Drug absorption in pharmacokinetics is the process by which a drug enters the bloodstream from its site of administration. Absorption happens when a drug travels from the site of administration to the systemic circulation—which provides functional blood supply to all body tissues. The rate and extent of absorption determine the drug’s bioavailability and onset of action.
Drug absorption in pharmacokinetics is the process by which a drug enters the bloodstream from its site of administration. Absorption happens when a drug travels from the site of administration to the systemic circulation—which provides functional blood supply to all body tissues. The rate and extent of absorption determine the drug’s bioavailability and onset of action.
2.1 Mechanisms of Drug Absorption
Drugs cross biological membranes through several mechanisms:
- Passive diffusion – Most common mechanism; drugs move from high to low concentration down a concentration gradient. This process does not require energy and is the primary mechanism for most drugs.
- Facilitated diffusion – Carrier-mediated transport down a concentration gradient, not requiring energy. This mechanism is saturable and specific for certain molecules.
- Active transport – Carrier-mediated transport against a concentration gradient, requiring energy (ATP). This mechanism enables absorption of certain drugs against concentration gradients.
- Pinocytosis – Engulfment of drug particles by cell membranes, a minor mechanism for drug absorption.
2.2 Key Factors Affecting Drug Absorption
| Factor | Impact on Absorption | Clinical Relevance |
|---|---|---|
| Route of administration | Oral, IV, IM, SC, transdermal, inhalation | IV provides 100% bioavailability; oral absorption varies |
| Drug solubility | Lipid-soluble drugs absorb more readily | Lipophilic drugs have better oral absorption |
| Gastric pH | Affects drug ionization and solubility | Weak acids absorb in stomach; weak bases in intestine |
| Surface area | Small intestine has large surface area | Major site for drug absorption |
| Blood flow | Increased blood flow enhances absorption | Exercise, fever can alter absorption |
| First-pass metabolism | Liver metabolism reduces bioavailability | Significant for drugs like propranolol, morphine |
| Food effects | Can alter absorption rate and extent | High-fat meals increase lipophilic drug absorption |
2.3 Bioavailability: The Critical Measure
The extent of absorption into the bloodstream can be described by bioavailability, which is defined as the fraction of drug that reaches systemic circulation.
- Oral drugs often pass through the small intestine and liver, where some amount of the drug is eliminated prior to reaching the bloodstream (first-pass metabolism), resulting in decreased bioavailability.
- Intravenous drugs are delivered directly to the bloodstream and have 100% bioavailability.
- Other routes (sublingual, transdermal, inhalation) bypass first-pass metabolism to varying degrees.
The FDA emphasizes that important absorption information communicated in drug labeling includes bioavailability, time to reach maximum concentration (Tmax), and the effect of food on absorption.
3. Drug Distribution
Drug distribution in pharmacokinetics refers to the movement of drug molecules from the bloodstream to tissues and organs. After absorption, the drug distributes throughout the body via the systemic circulation. The extent and pattern of distribution determine drug concentration at target sites and potential toxicity in other tissues.
3.1 Determinants of Drug Distribution
Drug distribution depends on several interrelated factors:
- Blood flow to tissues – Highly perfused organs (brain, heart, liver, kidneys) receive drug more rapidly than poorly perfused tissues (bone, adipose).
- Plasma protein binding – Only free (unbound) drug is pharmacologically active and available for distribution to tissues. Drugs that are highly protein-bound (>90%) have limited distribution and reduced clearance.
- Lipid solubility – Lipophilic drugs cross cell membranes more easily, leading to more extensive tissue distribution and larger volumes of distribution.
- Tissue permeability – Capillary structure varies between tissues, affecting drug passage. Fenestrated capillaries in the liver and kidney allow easier passage than continuous capillaries in muscle and brain.
- Volume of distribution (Vd) – A numerical descriptor of a drug’s propensity to either remain in blood or distribute to various organs throughout the body. High Vd indicates extensive tissue distribution.
3.2 Important Barriers in Drug Distribution
- Blood-brain barrier (BBB) – Tight junctions in brain capillaries restrict entry of many drugs. Only lipid-soluble drugs or those with specific transport mechanisms cross the BBB effectively.
- Placental barrier – Limits fetal exposure to certain drugs, though many drugs cross the placenta to some degree. This has important implications for prescribing during pregnancy.
- Blood-testis barrier – Restricts drug entry into reproductive tissues, protecting germ cells.
3.3 Clinical Significance of Drug Distribution
Distribution determines:
- Drug concentration at the target site – Essential for therapeutic effect
- Duration of action – Drugs with high Vd have prolonged elimination
- Potential toxicity – Drugs that cross the BBB may cause CNS effects; accumulation in adipose tissue may prolong effects
Highly lipid-soluble drugs can cross the blood-brain barrier easily, making them effective in CNS disorders. The percentage of protein binding and volume of distribution are typically communicated in drug labeling and guide dosing in conditions like hypoalbuminemia.
4. Drug Metabolism
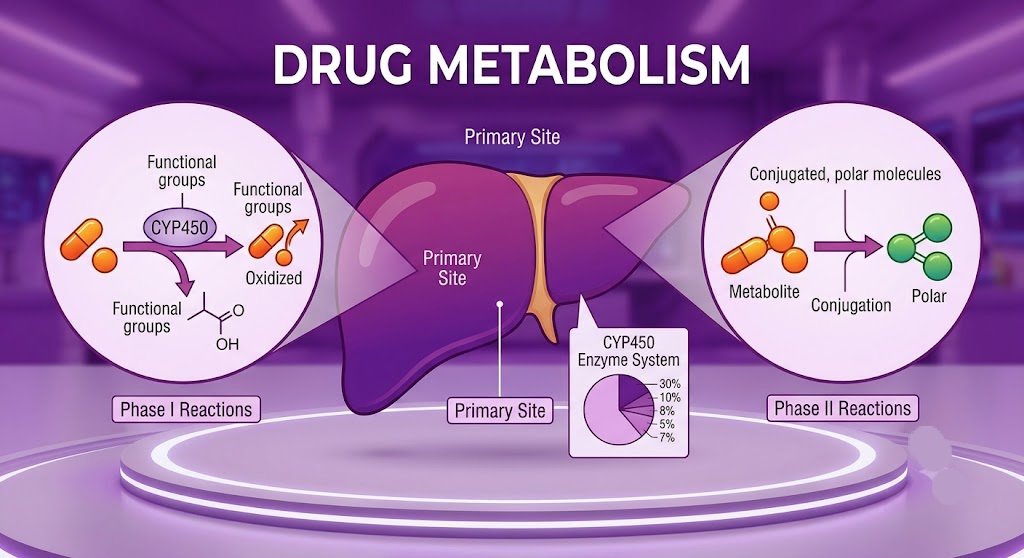 Drug metabolism in pharmacology is the biochemical modification of drugs, mainly in the liver, to make them more water-soluble for elimination. Metabolism converts lipophilic molecules into more hydrophilic ones so they can be excreted by the kidneys or bile. The process involves enzymatic reactions that alter the drug’s chemical structure, typically resulting in pharmacological inactivation, though some drugs (prodrugs) require metabolism to become active.
Drug metabolism in pharmacology is the biochemical modification of drugs, mainly in the liver, to make them more water-soluble for elimination. Metabolism converts lipophilic molecules into more hydrophilic ones so they can be excreted by the kidneys or bile. The process involves enzymatic reactions that alter the drug’s chemical structure, typically resulting in pharmacological inactivation, though some drugs (prodrugs) require metabolism to become active.
4.1 Sites of Drug Metabolism
- Liver – Primary site of metabolism, containing the highest concentration of drug-metabolizing enzymes
- Intestines – Significant first-pass metabolism occurs in intestinal epithelium
- Kidneys – Some metabolic capacity, particularly for peptide drugs
- Plasma – Certain enzymes in blood (e.g., esterases, pseudocholinesterase)
- Lungs – Metabolism of certain drugs, including some inhaled anesthetics
4.2 Phases of Drug Metabolism
Phase I Reactions (Functionalization Reactions)
These reactions introduce or expose a functional group on the drug molecule, making it more polar:
- Oxidation – Most common Phase I reaction, mediated primarily by cytochrome P450 (CYP450) enzymes. Involves the addition of oxygen or removal of hydrogen.
- Reduction – Addition of electrons, often mediated by reductases in the liver and intestinal microflora.
- Hydrolysis – Cleavage of bonds using water, mediated by esterases and amidases.
Phase II Reactions (Conjugation Reactions)
These reactions attach a polar molecule to the drug or its Phase I metabolite, further increasing water solubility:
- Glucuronidation – Most common Phase II reaction, catalyzed by UGT enzymes; attaches glucuronic acid
- Sulfation – Addition of sulfate group, catalyzed by sulfotransferases (SULTs)
- Acetylation – Addition of acetyl group, catalyzed by N-acetyltransferases (NATs); genetically polymorphic
- Methylation – Addition of methyl group, catalyzed by methyltransferases
- Glutathione conjugation – Important for detoxification of reactive electrophiles
4.3 The Cytochrome P450 System
The CYP450 enzyme system is the most important family of drug-metabolizing enzymes. According to a study of the 100 most prescribed drugs:
| CYP450 Enzyme | Number of Drugs Metabolized | Clinical Significance |
|---|---|---|
| CYP3A4/5 | 43 drugs | Most important CYP; involved in 50% of drug metabolism |
| CYP2D6 | 23 drugs | Highly polymorphic; poor metabolizers at risk |
| CYP2C9 | 23 drugs | Metabolizes warfarin, NSAIDs; genetic variability |
| CYP2C19 | 22 drugs | Metabolizes clopidogrel, proton pump inhibitors |
| CYP1A2 | 14 drugs | Induced by smoking, affected by caffeine |
| CYP2C8 | 11 drugs | Metabolizes repaglinide, paclitaxel |
4.4 Clinical Importance of Drug Metabolism
- Activates prodrugs – Some drugs require metabolism to become therapeutically active (e.g., clopidogrel, codeine, tamoxifen)
- Inactivates drugs – Most drugs are inactivated by metabolism, limiting their duration of action
- Produces toxic metabolites – Some metabolites are toxic (e.g., acetaminophen NAPQI, which can cause hepatotoxicity)
- Affects drug half-life and clearance – Rate of metabolism determines how quickly a drug is eliminated
- Determines drug-drug interactions – Inhibition or induction of CYP450 enzymes can significantly alter drug concentrations
The FDA notes that important metabolism and excretion information communicated in drug labeling includes half-life (T1/2), major route of elimination, and percentage excreted in urine or feces.
5. Drug Excretion
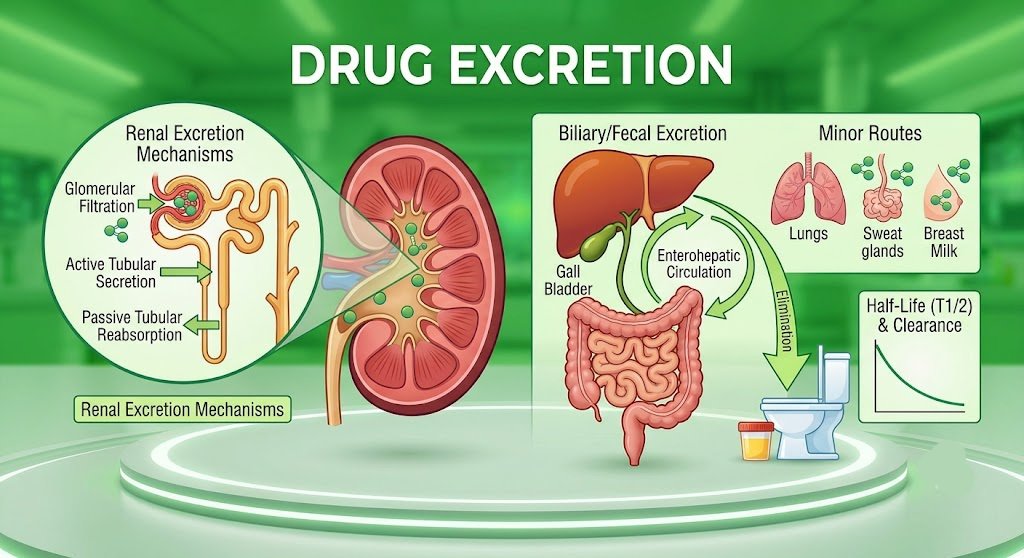 Drug excretion in pharmacology is the removal of drugs and metabolites from the body. Drug excretion is the irreversible loss of drug from the body and is the final step in the ADME process. The rate of excretion determines drug duration and guides dose adjustment in organ dysfunction.
Drug excretion in pharmacology is the removal of drugs and metabolites from the body. Drug excretion is the irreversible loss of drug from the body and is the final step in the ADME process. The rate of excretion determines drug duration and guides dose adjustment in organ dysfunction.
5.1 Major Routes of Drug Excretion
| Route | Description | Importance | Factors Affecting |
|---|---|---|---|
| Renal (urine) | Excretion via kidneys | Most important route for most drugs | Renal function, pH, drug protein binding |
| Biliary (feces) | Excretion via bile into intestines | Significant for some drugs and metabolites | Liver function, enterohepatic circulation |
| Pulmonary (lungs) | Excretion of volatile gases | Minor route for most drugs | Respiratory rate, drug volatility |
| Sweat | Excretion in sweat | Minor route; variable between individuals | Body temperature, physical activity |
| Saliva | Excretion in saliva | Minor route; used for therapeutic drug monitoring | Salivary pH, drug lipophilicity |
| Breast milk | Excretion in milk | Important for nursing mothers | Drug lipophilicity, protein binding, milk pH |
5.2 Renal Excretion Mechanisms
The kidney excretes drugs through three processes:
- Glomerular filtration – Free (unbound) drug passes through glomerular capillaries into the filtrate. Only the unbound fraction is filtered, making protein binding an important determinant of renal clearance.
- Active tubular secretion – Transporters (OAT, OCT, P-gp) actively secrete drugs from blood into the tubule, independently of protein binding. This process is saturable and can be a site of drug-drug interactions.
- Passive tubular reabsorption – Some drug is reabsorbed back into circulation from the tubule. This is influenced by drug ionization, pH, and lipid solubility.
5.3 Enterohepatic Circulation
Drugs appearing in bile enter the intestines and may be reabsorbed, resulting in enterohepatic circulation. This can prolong drug action, cause a secondary peak in plasma concentration, and complicate dosing. Examples of drugs with significant enterohepatic circulation include:
- Warfarin
- Morphine
- Digoxin
- Estrogens
5.4 Half-Life and Clearance
- Half-life (t1/2) – The time needed for the drug’s concentration to be halved. It is determined by both distribution and elimination processes.
- Steady state – Achieved after approximately four to five half-lives. At steady state, drug input equals drug elimination, and plasma concentrations remain relatively constant.
- Clearance – A measure of the body’s ability to eliminate a drug, defined as the volume of blood completely cleared of drug per unit time (mL/min). Clearance is additive across elimination organs.
5.5 Clinical Importance of Drug Excretion
- Determines drug duration of action – Prolonged half-life means longer duration
- Prevents toxicity – Elimination maintains drug concentrations within the therapeutic window
- Guides dose adjustment – Patients with renal or hepatic impairment require dose reduction or extended intervals
- Influences drug interactions – Competition for renal transporters can alter drug clearance
In renal failure, the half-life of drugs may be prolonged due to reduced clearance, requiring widening of the dosage interval. For drugs with a narrow therapeutic index, such as digoxin, this has serious clinical consequences.
6. The ADME Process in Drugs Explained Step-by-Step
The complete drug absorption distribution metabolism excretion system works in a coordinated manner:
- Drug is administered – Via oral, intravenous, intramuscular, subcutaneous, or other routes
- Absorbed into bloodstream – From the site of administration into systemic circulation
- Distributed to tissues – Via systemic circulation to target and non-target tissues
- Metabolized – Mainly in the liver, but also in other tissues, converting lipophilic drugs to hydrophilic metabolites
- Excreted – Via kidneys, bile, or other routes, eliminating the drug from the body
6.1 Mathematical Models in ADME
Modern pharmacology uses sophisticated modeling to predict ADME properties. In silico modelling of drug disposition involves absorption, distribution, and excretion processes, and includes thorough knowledge of various database expeditions, molecular docking studies, and quantitative structure-activity relationships (QSAR) evaluation. Physiologically-based pharmacokinetic (PBPK) modeling considers the complex interplay between physiological parameters and drug-related characteristics relating to absorption and metabolism.
The primary development in ADMET modeling has been the clarification of the function and effective modeling of various transporters. These developments hasten the transition of model construction from computational to experimental scientists, enabling earlier prediction of drug disposition in humans.
6.2 The Plasma Concentration-Time Curve
The ADME process determines the plasma concentration-time curve, which is critical for safe and effective drug therapy. Key parameters derived from this curve include:
- Cmax – Maximum plasma concentration
- Tmax – Time to reach maximum concentration
- AUC – Area under the curve (total drug exposure)
- t1/2 – Half-life (elimination rate)
- Clearance – Rate of drug removal
7. Clinical Importance of ADME Pharmacokinetics
Understanding ADME pharmacokinetics explained is essential in medical practice because it helps:
7.1 Optimize Drug Dosing
Pharmacokinetic principles help determine:
- Loading doses – To rapidly achieve therapeutic concentrations
- Maintenance doses – To sustain therapeutic concentrations
- Dosing intervals – To maintain concentrations within the therapeutic window
- Duration of therapy – To achieve desired outcomes while minimizing toxicity
The FDA emphasizes that clinical pharmacologists help determine “how much to give” and “how often to give it” during drug development and clinical practice.
7.2 Avoid Toxicity
Understanding ADME helps:
- Predict drug accumulation – In patients with organ dysfunction
- Identify patients at risk – For toxicity due to genetic or physiological factors
- Adjust doses – In organ dysfunction to prevent drug accumulation
- Establish therapeutic windows – To guide safe prescribing
7.3 Predict Drug Interactions
ADME characterization enables preliminary assessment of potential drug-drug interaction liabilities, which may be critical when it comes to patient selection and safety. The characterization of a drug’s ADME profile is crucial for accurately determining its safety and efficacy.
Drug interactions can occur at any stage of the ADME process:
- Absorption – Altered gastric pH, motility, or chelation
- Distribution – Competition for protein binding
- Metabolism – CYP450 inhibition or induction
- Excretion – Competition for renal or biliary transporters
7.4 Adjust Therapy in Special Populations
| Population | ADME Considerations | Clinical Implications |
|---|---|---|
| Elderly | Reduced renal function, altered metabolism, changes in body composition | Lower doses, increased monitoring |
| Children | Immature metabolic pathways, different body composition | Weight-based dosing, careful monitoring |
| Pregnancy | Altered absorption, distribution, metabolism, excretion | Dose adjustments, careful drug selection |
| Renal failure | Reduced excretion, require dose adjustment | Extended intervals, reduced doses |
| Hepatic failure | Reduced metabolism, increased toxicity risk | Reduced doses, avoid hepatotoxic drugs |
| Obesity | Altered distribution, variable clearance | Dosing based on ideal body weight |
7.5 Improve Therapeutic Outcomes
ADME and PK characterization form an integral part of the drug discovery and development process for all new drugs. Pathophysiological disorders that affect any stage of this process can impact the time concentration curve of the medicine and, thus, efficacy and toxicity.
8. Factors Affecting the ADME Process
Several physiological and pathological factors influence the ADME process in drugs explained:
8.1 Genetic Factors
Large interindividual variations in drug response can arise from multiple genetic factors affecting drug absorption, distribution, biotransformation, excretion, interaction with receptor sites, or combinations of these. Genetic polymorphisms in genes that encode drug-metabolizing enzymes or drug transporters (e.g., CYP2D6, CYP2C9, and CYP2C19) significantly affect drug disposition.
8.2 Age
Elderly patients experience physiologic changes that affect many aspects of pharmacokinetics:
- Reduced renal function (decreased GFR)
- Altered liver metabolism (reduced Phase I metabolism)
- Changes in body composition (increased fat, decreased water)
- Decreased plasma protein binding (hypoalbuminemia)
Children have immature metabolic and excretory pathways, affecting drug handling. Pediatric dosing must account for developmental changes in absorption, distribution, metabolism, and excretion.
8.3 Liver Function
Liver disease affects drug metabolism, increasing toxicity risk. Hepatic impairment can:
- Reduce Phase I and Phase II metabolism
- Increase bioavailability of oral drugs (reduced first-pass effect)
- Prolong drug half-life
- Increase risk of drug accumulation and toxicity
- Reduce plasma protein binding (due to decreased albumin synthesis)
8.4 Kidney Function
Patients with kidney failure require dose reduction due to decreased excretion. Renal impairment affects:
- Glomerular filtration rate (GFR) – reduced clearance
- Tubular secretion – reduced active transport
- Drug clearance – prolonged half-life
- Drug accumulation and toxicity – increased risk
8.5 Pregnancy
Hormonal status during pregnancy affects:
- Gastric emptying (affects absorption) – delayed gastric emptying
- Plasma volume expansion (affects distribution) – increased Vd
- Hepatic enzyme induction (affects metabolism) – increased clearance
- Increased renal blood flow (affects excretion) – increased renal clearance
8.6 Drug Interactions
Drug-drug interactions can affect ADME through:
- CYP450 enzyme inhibition or induction
- Competition for plasma protein binding
- Competition for renal tubular secretion
- Alteration of gastrointestinal motility
- Changes in gastric pH
8.7 Diet and Alcohol
- Food – Can affect absorption rate and extent, particularly for lipophilic drugs
- Alcohol – Can affect liver metabolism and gastric emptying
- Grapefruit juice – Inhibits CYP3A4, affecting drug metabolism and increasing bioavailability of many drugs
- High-fat meals – Can increase absorption of lipophilic drugs
- Protein intake – Affects plasma protein binding and drug distribution
8.8 Sex
Sex differences affect:
- Body composition (affects distribution) – women have higher body fat percentage
- Hepatic enzyme activity – some CYP enzymes are sex-dependent
- Renal function – women typically have lower GFR
- Hormonal influences on drug metabolism and excretion
9. Pharmacokinetics Summary of ADME
The ADME pharmacokinetics explained model is the foundation of modern pharmacology:
| Process | Definition | Key Determinants | Clinical Impact |
|---|---|---|---|
| Absorption | Drug entry into bloodstream | Route, solubility, pH, blood flow, first-pass effect | Bioavailability, onset of action |
| Distribution | Movement to tissues | Blood flow, protein binding, lipid solubility, barriers | Site of action, duration, toxicity |
| Metabolism | Chemical modification | Liver function, CYP450 enzymes, genetics, age | Activation, inactivation, clearance, interactions |
| Excretion | Elimination from body | Renal function, biliary excretion, half-life | Duration, toxicity prevention, dose adjustment |
Together, these processes control:
- Drug concentration – at the site of action
- Duration of action – how long the drug works
- Safety and effectiveness – therapeutic index
- Drug interactions – potential for altered ADME
10. Clinical Case Scenarios
Case 1: Renal Impairment and Drug Dosing
Presentation: A 72-year-old female with chronic kidney disease (eGFR 25 mL/min) is prescribed a renally eliminated drug. Standard dosing would lead to drug accumulation and toxicity.
ADME Consideration: Reduced renal clearance due to impaired kidney function.
Management:
- Reduce dose by 50% or extend dosing interval
- Monitor drug levels (if available)
- Consider alternative drug with non-renal elimination
Rationale: Drug excretion is primarily renal. In renal failure, clearance is reduced, requiring dose adjustment to prevent toxicity.
Case 2: Genetic Polymorphism (CYP2D6)
Presentation: A 45-year-old patient on codeine for pain reports no pain relief despite standard dosing. The patient is later found to be a CYP2D6 poor metabolizer.
ADME Consideration: Codeine is a prodrug requiring CYP2D6-mediated metabolism to morphine for analgesic effect.
Management:
- Discontinue codeine
- Switch to an alternative analgesic not requiring CYP2D6 metabolism
- Consider pharmacogenetic testing for future prescribing
Rationale: Genetic polymorphisms affect drug metabolism. Poor metabolizers derive no benefit from prodrugs requiring CYP2D6 activation.
Case 3: Drug-Drug Interaction
Presentation: A 60-year-old patient on warfarin for atrial fibrillation is prescribed fluconazole for a fungal infection. The patient’s INR rises significantly, and bleeding is observed.
ADME Consideration: Fluconazole inhibits CYP2C9, the enzyme responsible for metabolizing warfarin.
Management:
- Reduce warfarin dose or discontinue warfarin
- Switch to a different antifungal (less CYP interaction)
- Monitor INR closely
Rationale: CYP450 inhibition reduces drug metabolism, increasing concentrations of the affected drug and risk of toxicity.
Case 4: First-Pass Metabolism
Presentation: A patient receives a sublingual dose of nitroglycerin for acute angina. The drug acts rapidly with high bioavailability.
ADME Consideration: Sublingual administration bypasses first-pass metabolism in the liver, providing 100% bioavailability and rapid onset.
Rationale: Drugs administered sublingually, transdermally, or rectally bypass the portal circulation and avoid first-pass metabolism.
Case 5: Hepatic Impairment
Presentation: A patient with cirrhosis requires therapy for a chronic condition. The drug is extensively metabolized by the liver.
ADME Consideration: Reduced liver function decreases drug metabolism, prolonging half-life and increasing toxicity risk.
Management:
- Reduce dose or extend dosing interval
- Choose a drug with less hepatic metabolism
- Monitor for signs of toxicity
Rationale: Hepatic impairment reduces the liver’s capacity to metabolize drugs, requiring dose adjustment to prevent accumulation.
The ADME pharmacokinetics explained framework provides the essential foundation for understanding how drugs move through and are processed by the human body. The four processes—Absorption, Distribution, Metabolism, and Excretion—work in concert to determine a drug’s concentration at its site of action, its duration of effect, and its ultimate elimination from the body.
The evidence-based principles of ADME pharmacokinetics demonstrate that:
- Absorption determines drug entry and bioavailability—critical for drug selection and route of administration.
- Distribution determines drug concentration at target sites—essential for understanding duration of action and potential toxicity.
- Metabolism transforms drugs for elimination—critical for drug interactions and genetic variability.
- Excretion removes drugs from the body—essential for dose adjustment in renal and hepatic impairment.
For healthcare professionals, understanding ADME is critical for:
- Prescribing safe and effective drug therapy – Selecting appropriate drugs and doses
- Adjusting doses in patients with organ dysfunction – Preventing toxicity in renal and hepatic impairment
- Predicting and managing drug interactions – Identifying CYP450 interactions and transporter-mediated interactions
- Optimizing treatment outcomes – Achieving therapeutic concentrations while minimizing adverse effects
For patients, ADME principles explain why medications are taken at specific times, with or without food, and why certain health conditions may require dose adjustments. Understanding these principles empowers patients to use medications safely and effectively.
The integration of ADME principles into clinical practice—from drug discovery through therapeutic drug monitoring—represents one of the most important advances in modern medicine. As computational and modeling techniques continue to evolve, our ability to predict and optimize drug behavior in individual patients will only improve, leading to more personalized and effective pharmacotherapy.
Disclaimer: This comprehensive clinical guide is intended for educational purposes only. It does not replace clinical judgment or individual patient assessment. Always follow local guidelines and individual patient factors when making treatment decisions. Consult drug interactions and current prescribing information before initiating therapy.
Last Updated: July 2026 | Version: 2.0 | Review Frequency: Annual review recommended
The evidence-based answer to “What is the ADME process in pharmacology?” is a comprehensive framework that every healthcare professional must master. Understanding these principles is essential for rational prescribing and optimal patient care.
For medical, pharmacy, and dental students, mastering the ADME framework is essential for providing safe, effective, and evidence-based pharmacotherapy. The key principles to remember are:
- Understand the drug – Its physicochemical properties determine ADME characteristics
- Understand the patient – Genetic, physiological, and pathological factors affect ADME
- Anticipate interactions – ADME is affected by concomitant medications and food
- Monitor and adjust – Individualize therapy based on response and organ function
- Communicate clearly – Explain ADME principles to patients in understandable terms
By adhering to these evidence-based principles, healthcare professionals can optimize drug therapy, minimize adverse effects, and improve patient outcomes while contributing to the broader goals of precision medicine and pharmacovigilance.
13. References
1. Allucent. What is Pharmacokinetics and ADME? 2024.
2. FDA. Clinical Pharmacology: Early Drug Development. 2024.
3. Johnson DB, et al. Exploring Computational Advancements in ADME: Essential Insights for Drug Disposition. Zhongguo Ying Yong Sheng Li Xue Za Zhi. 2024;40:e20240017.
4. In Silico ADME Methods Used in the Evaluation of Natural Products. Pharmaceutics. 2025.
5. Drug metabolism and drug transport of the 100 most prescribed oral drugs. Basic & Clinical Pharmacology & Toxicology. 2022.
6. ScienceDirect. Drug Excretion – an overview. 2024.
7. Physiological factors affecting drug toxicity – PubMed. 2023.
8. Merck Manual Professional Edition. Overview of Pharmacokinetics. 2025.
9. Cytochrome P450 Enzymes. StatPearls. 2025.
10. Physiologically Based Pharmacokinetic Modeling. Clinical Pharmacology & Therapeutics. 2024.
11. Drug Interactions: Principles and Practice. Australian Prescriber. 2024.
12. Pharmacogenetics in Clinical Practice. New England Journal of Medicine. 2023.
Facebook Copyright Issues Solution 2026
SSTHEM.COM – Learn World Religions, History & Educational Knowledge
·
Health & Beauty Tips
This article has been written with a focus on evidence-based pharmacology, clinical pharmacokinetics, and practical application for medical, pharmacy, and dental students. The content aligns with FDA guidance, contemporary clinical pharmacology principles, and rational prescribing practices.