The Shocking Truth 2026 About Bioavailability Every Clinician Must Know
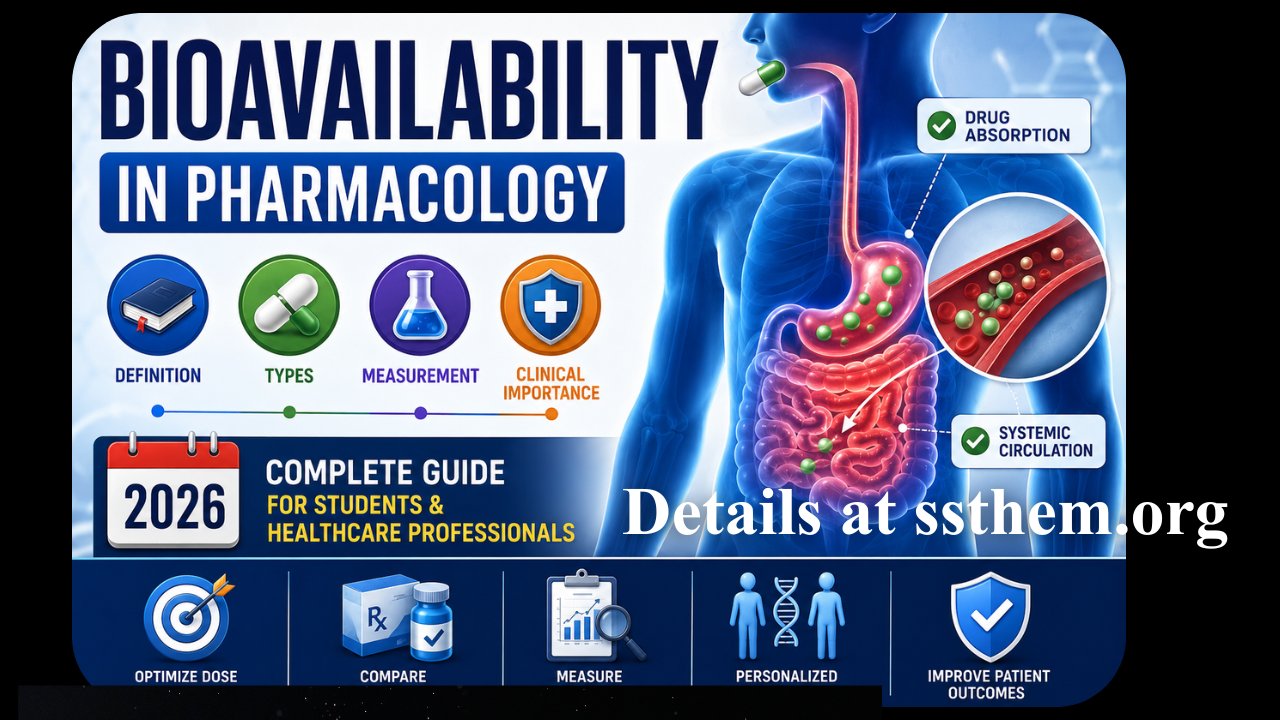
Bioavailability in Pharmacology: Definition, Types, Measurement, and Clinical Importance (2026)
Pharmacokinetics—the study of how the body affects a drug—rests upon four fundamental processes: absorption, distribution, metabolism, and excretion. Among these, bioavailability represents the most critical determinant of therapeutic efficacy, serving as the gateway through which drug molecules enter systemic circulation and ultimately reach their sites of action.
The clinical significance of bioavailability cannot be overstated. A drug, regardless of its pharmacological potency, is therapeutically useless if it cannot achieve sufficient concentrations at its target site. Bioavailability determines both the rate and extent to which an administered drug reaches systemic circulation, directly influencing dosing decisions, drug development, and patient outcomes.
The oral route remains the most common method of drug administration, yet oral bioavailability is influenced by a complex interplay of physicochemical properties (pKa, lipophilicity, solubility), pharmaceutical factors (dosage form design), and physiological conditions (gastrointestinal pH, gastric emptying, intestinal transit, metabolic activity).
This comprehensive article examines bioavailability from its fundamental definition through its clinical applications, providing healthcare professionals, students, and researchers with an evidence-based understanding of this cornerstone of pharmacotherapy.
Table of Contents
- 1. What Is Bioavailability?
- 2. Historical Background
- 3. Importance in Clinical Pharmacology
- 4. Types of Bioavailability
- 5. Factors Affecting Drug Bioavailability
- 6. Drug Formulation Factors
- 7. Patient Factors
- 8. First-Pass Metabolism
- 9. Drug Absorption and Bioavailability
- 10. Oral vs IV Bioavailability
- 11. Measurement and Calculation
- 12. Bioavailability Formula
- 13. Bioequivalence
- 14. Clinical Applications
- 15. Examples of Medicines with High and Low Bioavailability
- 16. Food–Drug Interactions
- 17. Disease Conditions Affecting Bioavailability
- 18. Special Populations
- 19. Advantages and Limitations
- 20. Common Misconceptions
- 21. Recent Clinical Research
- 22. Frequently Asked Questions
- 23. Key Takeaways
- 24. References
1. What Is Bioavailability?
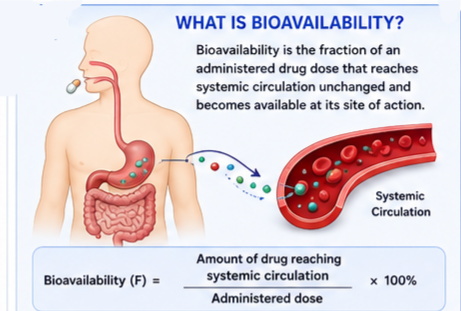 Bioavailability is the fraction of an administered drug dose that reaches systemic circulation unchanged and becomes available at its site of action. More precisely, it measures both the rate and extent of drug absorption into the bloodstream.
Bioavailability is the fraction of an administered drug dose that reaches systemic circulation unchanged and becomes available at its site of action. More precisely, it measures both the rate and extent of drug absorption into the bloodstream.
The concept is represented by the symbol “F” (from “fraction”) and is typically expressed as a percentage. For example, a drug with 70% bioavailability means that 70% of the administered dose successfully enters systemic circulation. The remaining 30% may be lost through incomplete absorption, metabolism, or excretion before reaching the bloodstream.
Formal Definition
“The rate and extent to which the active ingredient or active moiety is absorbed from a drug product and becomes available at the site of action.” — FDA
Two Key Components of Bioavailability
| Component | Description | Clinical Significance |
|---|---|---|
| Extent | The total amount of drug that reaches systemic circulation | Determines the overall dose required for therapeutic effect |
| Rate | The speed at which the drug reaches systemic circulation | Influences onset of action and peak plasma concentrations |
It is important to distinguish bioavailability from absorption. While absorption refers to the movement of a drug from its administration site into the bloodstream, bioavailability accounts for losses that occur during this process—including metabolism before the drug reaches systemic circulation.
2. Historical Background
The concept of bioavailability emerged in the mid-20th century as pharmacologists recognized that different formulations of the same drug could produce different therapeutic effects despite containing identical active ingredients. Early bioavailability studies in the 1960s and 1970s revealed that factors such as tablet formulation, particle size, and manufacturing processes significantly influenced drug absorption.
A landmark publication by Weber et al. (1975) described bioavailability as “the actual percentage of a drug released from the dosage form, which reaches the receptor site in sufficient quantity to induce a biological effect”. This definition highlighted that drug efficacy depends not only on the drug’s pharmacological properties but also on its ability to reach the target site.
The concept gained regulatory importance as generic drug manufacturing expanded, requiring evidence that substitute formulations provide equivalent therapeutic effects. The FDA has been the international leader in guiding bioavailability and bioequivalence studies since the early 1980s, when the US Congress passed laws allowing for the approval of drugs based on bioequivalence data.
3. Importance in Clinical Pharmacology
Bioavailability is fundamental to pharmacokinetics—the study of drug movement through the body. Pharmacokinetics is often represented by the acronym ABCD:
- Administration: Route and dosing
- Bioavailability: Fraction reaching systemic circulation
- Clearance: Removal of active drug from systemic circulation
- Distribution: Movement of drug to body compartments
Understanding bioavailability allows clinicians to:
- Select appropriate routes of administration based on therapeutic goals
- Adjust dosages for patients with conditions affecting absorption or metabolism
- Predict drug interactions that may alter bioavailability
- Evaluate generic drug equivalence to branded products
Oral drug administration accounts for approximately 90% of the global market share of clinically administered drugs. While this route is the most convenient, limited and variable bioavailability can complicate achieving the desired clinical effect. Over 90% of pharmaceuticals are known to have limitations on their oral bioavailability.
4. Types of Bioavailability
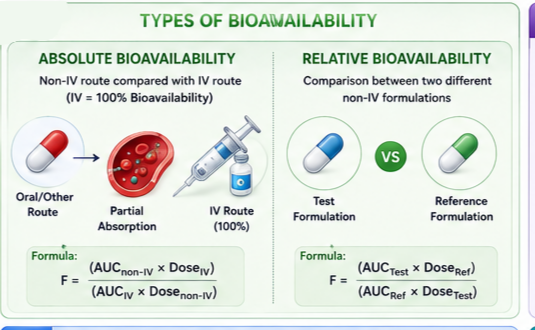 Bioavailability is categorized into two primary types: absolute and relative. Both are essential for understanding drug performance but serve different comparative purposes.
Bioavailability is categorized into two primary types: absolute and relative. Both are essential for understanding drug performance but serve different comparative purposes.
4.1 Absolute Bioavailability
Absolute bioavailability compares the bioavailability of a drug administered via a non-intravenous route (such as oral, subcutaneous, or intramuscular) to the same drug administered intravenously.
The intravenous route serves as the reference standard because a drug delivered directly into the bloodstream achieves 100% bioavailability—there is no loss through absorption barriers or first-pass metabolism.
Calculation formula:
Absolute Bioavailability (F) = (AUCnon-IV × DoseIV) ÷ (AUCIV × Dosenon-IV)
Where AUC represents the area under the plasma concentration–time curve.
Clinical relevance:
- Determines whether a drug is suitable for oral administration
- Guides dose conversion between IV and oral routes
- Identifies drugs requiring alternative administration routes due to poor oral absorption
4.2 Relative Bioavailability
Relative bioavailability compares the bioavailability of two different non-intravenous formulations of the same drug. This comparison may involve:
- Different dosage forms (tablet vs. capsule vs. syrup)
- Same dosage form from different manufacturers (brand vs. generic)
- Different routes of administration (oral vs. sublingual vs. rectal)
Calculation formula:
Relative Bioavailability = (AUCTest × DoseReference) ÷ (AUCReference × DoseTest)
Clinical example: An asthma medication comparison: A patient receives either a tablet or inhaler containing the same active substance. If the inhalation formulation has a relative bioavailability of 167% compared to the tablet, more active drug reaches systemic circulation from the inhaler—likely due to the inhaler’s avoidance of first-pass metabolism.
5. Factors Affecting Drug Bioavailability
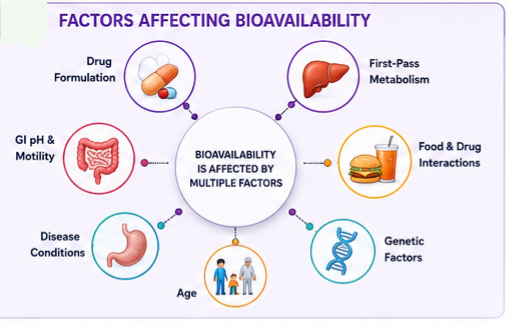
Multiple factors influence drug bioavailability, spanning drug formulation characteristics, patient physiology, genetic variability, and external variables.
Drug Formulation Factors
Physicochemical Properties: Active pharmaceutical ingredients (APIs) with poor water solubility limit their application. Various methods such as salt formation, amorphous solid dispersions, and cocrystals can be employed to overcome this challenge.
Dissolution and Particle Size: A drug must dissolve in gastrointestinal fluids before absorption can occur. Poorly soluble drugs may have limited and variable bioavailability, as time at the absorption site may be insufficient for complete dissolution. Particle size reduction can increase dissolution rate and improve bioavailability.
Chemical Stability: Some drugs degrade in the acidic gastric environment or are metabolized by digestive enzymes before reaching systemic circulation. The abundant peptidases and proteases in the GI tract can compromise drug stability.
Excipients and Formulation: Inactive ingredients in drug products can significantly influence absorption. Different formulations of the same active ingredient may produce different bioavailability profiles.
Complex Formation: Certain drugs form complexes that reduce absorption. For example, tetracycline binds to polyvalent metal ions (calcium, magnesium, iron), decreasing its bioavailability.
6. Drug Formulation Factors
Pharmaceutical formulation plays a critical role in determining drug bioavailability. Key formulation factors include:
| Formulation Factor | Impact on Bioavailability | Clinical Example |
|---|---|---|
| Particle size reduction | Increases surface area, enhancing dissolution and absorption | Micronized drug products (e.g., griseofulvin) |
| Salt formation | Improves aqueous solubility and dissolution rate | Sodium salts of weak acids |
| Crystal form (polymorph) | Different polymorphs have different solubility characteristics | Ritonavir polymorph conversion |
| Excipients | Can enhance or retard dissolution, affect GI motility | Surfactants, disintegrants, binders |
| Dosage form design | Solutions > suspensions > capsules > tablets (absorption speed) | Immediate-release vs. controlled-release |
Novel Formulation Approaches
Self-emulsifying drug delivery systems (SEDDS) act as a game-changer to overcome challenges and limitations of poor bioavailability. The development of multifunctional systems capable of combining controlled release, targeted delivery, and diagnostic capabilities is a promising avenue.
7. Patient Factors
Patient-specific factors significantly influence drug bioavailability:
Age
Age-related changes in GI function, liver metabolism, and body composition affect drug bioavailability. Neonates have higher gastric pH and slower gastric emptying; elderly patients may have reduced GI motility and splanchnic blood flow.
Genetic Factors
Polymorphisms in intestinal transporters and metabolic enzymes can create substantial inter-individual variability. For instance, genetic variations in P-glycoprotein transporters and cytochrome P450 enzymes influence drug absorption and metabolism.
Stress
Psychological and physiological stress can alter GI motility and absorption patterns.
Disease States
Gastrointestinal disorders (celiac disease, Crohn’s disease, bariatric surgery), liver disease, and renal impairment can significantly alter drug bioavailability.
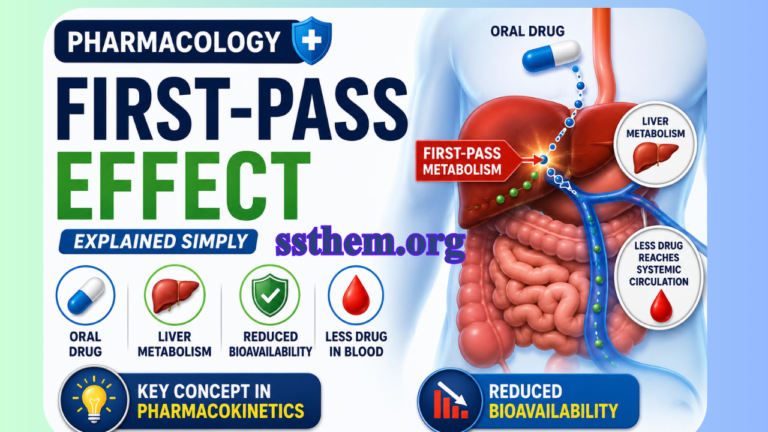
8. First-Pass Metabolism
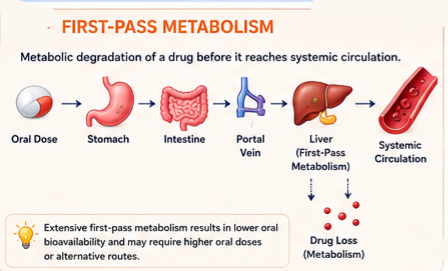 First-pass metabolism (also called presystemic metabolism) is the metabolic degradation of a drug before it reaches the systemic circulation. This primarily occurs in two locations:
First-pass metabolism (also called presystemic metabolism) is the metabolic degradation of a drug before it reaches the systemic circulation. This primarily occurs in two locations:
- Intestinal wall: Drug-metabolizing enzymes in the gut epithelium (particularly CYP3A4)
- Liver: Hepatic enzymes that metabolize drugs entering via the portal circulation
The liver is usually assumed to be the major site of first-pass metabolism of a drug administered orally, but other potential sites are the gastrointestinal tract, blood, vascular endothelium, lungs, and the arm from which venous samples are taken.
When several sites of first-pass metabolism are in series, the bioavailability is the product of the fractions of drug entering the tissue that escape loss at each site.
Clinical Consequences of Extensive First-Pass Metabolism
- Much larger oral doses than intravenous doses are required to achieve equivalent plasma concentrations
- For some drugs, extensive first-pass metabolism precludes their use as oral agents (e.g., lignocaine, naloxone, glyceryl trinitrate)
Drugs with Considerable First-Pass Metabolism
Alprenolol, amitriptyline, dihydroergotamine, 5-fluorouracil, hydralazine, isoprenaline (isoproterenol), lignocaine (lidocaine), lorcainide, pethidine (meperidine), mercaptopurine, metoprolol, morphine, neostigmine, nifedipine, pentazocine, and propranolol.
9. Drug Absorption and Bioavailability
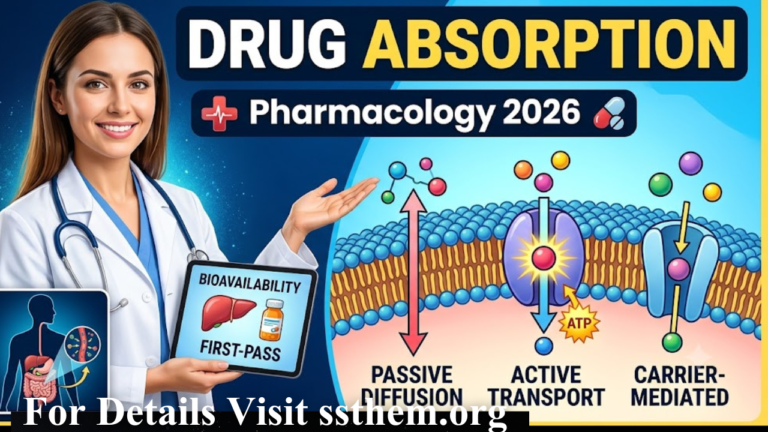
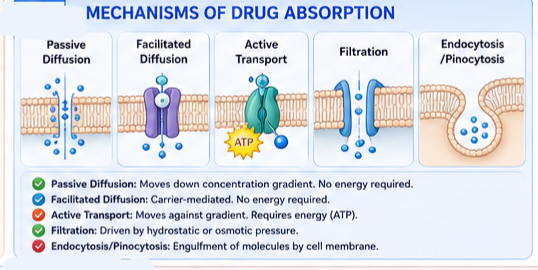 Drug absorption is the process by which drug molecules move from their site of administration into the bloodstream. The mechanisms of absorption include:
Drug absorption is the process by which drug molecules move from their site of administration into the bloodstream. The mechanisms of absorption include:
Passive Diffusion
The most common mechanism. Drug molecules move according to the concentration gradient—from higher to lower concentration—until equilibrium is reached. The rate is described by Fick’s Law of Diffusion. Lipid-soluble drugs diffuse most rapidly.
Facilitated Diffusion
Carrier-mediated transport that moves drugs down a concentration gradient without energy expenditure. Exhibits saturability and structural specificity.
Active Transport
Energy-consuming process that moves drugs against a concentration gradient. Essential for gastrointestinal absorption and renal and biliary excretion of many drugs.
Filtration
Passage of drugs through aqueous pores or intercellular spaces driven by hydrostatic or osmotic pressure. Primarily important for small water-soluble molecules.
Endocytosis and Pinocytosis
Engulfment of extracellular material by the cell membrane. Relatively unimportant for most drugs but relevant for very large molecules (proteins, peptides).
10. Oral vs IV Bioavailability
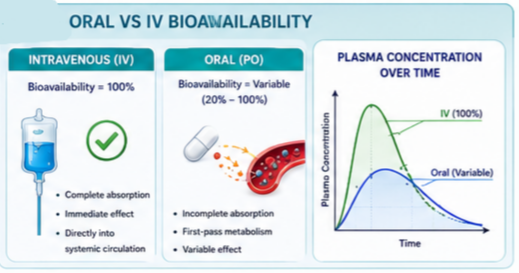
The route of administration fundamentally affects bioavailability:
| Route | Bioavailability | Advantages | Disadvantages |
|---|---|---|---|
| Intravenous (IV) | 100% | Immediate onset, complete bioavailability | Invasive, requires healthcare professional |
| Oral | Variable (typically 20–100%) | Convenient, non-invasive, economical | Variable absorption, first-pass metabolism |
| Sublingual | High (bypasses first-pass) | Rapid absorption, avoids hepatic metabolism | Limited to small lipophilic drugs |
| Rectal | Variable | Partial bypass of first-pass | Variable absorption, patient acceptability issues |
| Intramuscular (IM) | High (70–100%) | Rapid, avoids first-pass | Invasive, pain |
| Inhalational | High | Very rapid, avoids first-pass | Technique-dependent |
11. Measurement and Calculation
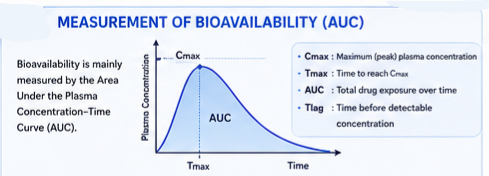
The AUC Concept
The area under the plasma concentration–time curve (AUC) is the most reliable measure of drug bioavailability. It represents the total drug exposure over time.
The plasma concentration–time curve is generated by:
- Administering a single dose of the drug
- Drawing blood samples at specific time intervals
- Measuring drug concentration in plasma
- Plotting concentration against time
| Parameter | Definition | Clinical Significance |
|---|---|---|
| Cmax | Maximum (peak) plasma concentration | Indicates extent of absorption |
| Tmax | Time to reach Cmax | Indicates rate of absorption |
| AUC | Total drug exposure over time | Measures overall bioavailability |
| Tlag | Time before detectable plasma concentrations | Reflects absorption delay |
12. Bioavailability Formula
The standard formula for calculating bioavailability using AUC data:
F = (AUCtest route × Dosereference) ÷ (AUCreference × Dosetest route)
For absolute bioavailability (IV as reference):
F = (AUCoral × DoseIV) ÷ (AUCIV × Doseoral)
Practical example: If a 100 mg oral dose produces an AUC of 50 mg·h/L, and a 50 mg IV dose produces an AUC of 80 mg·h/L:
- Dose-normalize the IV: 80 mg·h/L ÷ 50 mg = 1.6 mg·h/L per mg
- Expected oral AUC if 100% bioavailability: 100 mg × 1.6 = 160 mg·h/L
- Actual oral AUC: 50 mg·h/L
- F = 50 ÷ 160 = 0.3125 or 31.25% bioavailability
13. Bioequivalence
Bioequivalence indicates that two drug products (e.g., brand and generic) contain the same active ingredient and, when given to the same patient in the same dosage regimen, produce equivalent concentrations of drug in plasma and tissues.
Key Concepts
- Chemical equivalence: Same active compound in same amount; meets official standards
- Bioequivalence: Same rate and extent of absorption; essentially superimposable plasma concentration curves
- Therapeutic equivalence: Same therapeutic and adverse effects; expected when bioequivalence is established
Regulatory Requirements
The FDA recommends measurement of the parent drug released from the dosage form rather than the metabolite because the concentration-time profile of the parent drug is more sensitive to changes in formulation performance than the metabolite.
EMA recommends measurement of the parent compound as Cmax of a parent compound is usually more sensitive to differences between formulations with respect to the rate of absorption than Cmax of a metabolite.
14. Clinical Applications
Bioavailability has numerous clinical applications:
Dose Optimization
Determines appropriate dose for each route of administration. Drugs with low bioavailability may require higher oral doses or alternative routes.
Generic Drug Approval
Bioequivalence studies are required for generic drug approval, ensuring comparable therapeutic effects.
Drug-Drug Interaction Prediction
Identifying drugs that affect bioavailability of co-administered medications helps prevent adverse interactions.
Personalized Therapy
Understanding patient-specific factors enables individualized dose adjustments.
15. Examples of Medicines with High and Low Bioavailability
| Drug | Oral Bioavailability (%) | Reason |
|---|---|---|
| Warfarin | ~100% | Complete absorption, highly protein-bound |
| Doxycycline | ~90-100% | Well-absorbed, minimal food interaction |
| Metronidazole | ~100% | Complete oral absorption |
| Morphine | ~20-30% | Extensive first-pass metabolism |
| Propranolol | ~25-35% | Extensive first-pass metabolism |
| Labetalol | ~25% | First-pass metabolism |
| Insulin (oral) | 0% | Protein degradation; requires injection |
| Heparin (oral) | 0% | Degraded in GI tract; requires parenteral administration |
Clinical Example: Nitroglycerin
- Oral nitroglycerin: Extensive first-pass metabolism → low and variable bioavailability; used for prophylactic angina management
- Sublingual nitroglycerin: Bypasses first-pass metabolism → effects within 2 minutes; used for acute angina relief
16. Food–Drug Interactions
Concurrent food ingestion can significantly alter drug bioavailability:
Mechanisms
- Decreased absorption: Delayed gastric emptying, binding the drug, competition for transport systems
- Increased absorption: Enhanced dissolution (high-fat meals), inhibition of efflux transporters, altered GI pH
- Specific interactions: Tetracycline with dairy products (calcium binding), grapefruit juice with certain statins and calcium channel blockers (CYP3A4 inhibition)
| Drug | Food Effect | Mechanism |
|---|---|---|
| Tetracycline | Decreased absorption | Chelation with calcium, iron |
| Griseofulvin | Increased absorption | Enhanced dissolution with fatty meal |
| Isoniazid | Decreased absorption | Competition for absorption |
| Levothyroxine | Decreased absorption | Binding to food components |
| Itraconazole | Increased absorption | Enhanced dissolution with acidic beverage |
17. Disease Conditions Affecting Bioavailability
Gastrointestinal Disorders
- Malabsorption syndromes (celiac disease, Crohn’s disease): Reduced absorption surface area
- Achlorhydria: Altered gastric pH affecting dissolution of weakly acidic or basic drugs
- Bariatric surgery: Anatomical changes affecting drug absorption and dissolution
- Inflammatory bowel disease: Inflammation and altered motility can reduce bioavailability
Hepatic Impairment
Bile salt concentrations are reduced in patients with hepatic impairment, where duodenal bile salts are reduced by approximately two-fold. This can significantly impact the absorption of poorly soluble drugs.
Renal Disease
Impaired renal function decreases drug clearance, potentially increasing bioavailability and steady-state concentrations beyond expected levels. This is particularly important for drugs excreted primarily unchanged in urine.
Liver Disease
Reduced hepatic function can decrease first-pass metabolism, potentially increasing oral bioavailability and requiring dose adjustments.
18. Special Populations
Children
- Age-dependent differences in gastric pH, GI motility, and enzyme maturity
- Developmental changes in liver metabolism
- Bioavailability studies in children may use stable isotope methods to avoid repeated dosing
Pregnancy
- Altered GI motility and gastric emptying
- Changes in plasma volume and protein binding
- Potential effects on placental transfer and fetal exposure
Elderly
- Reduced GI motility and gastric acidity
- Decreased hepatic blood flow and metabolic capacity
- Reduced renal function
- Polypharmacy increasing drug–drug interaction risk
19. Advantages and Limitations
Advantages of Bioavailability Measurement
- Optimizes dosing: Determines appropriate dose for each route of administration
- Compares formulations: Evaluates generic drug equivalence
- Predicts interactions: Identifies drugs affecting bioavailability of co-administered medications
- Personalizes therapy: Enables dose adjustment for patient-specific factors
- Regulatory compliance: Supports drug approval and marketing authorization
Limitations of Current Models
- Assumes constant clearance: AUC calculations assume drug clearance remains constant between doses
- Assumes uniform distribution: In multi-compartment models, this may not hold
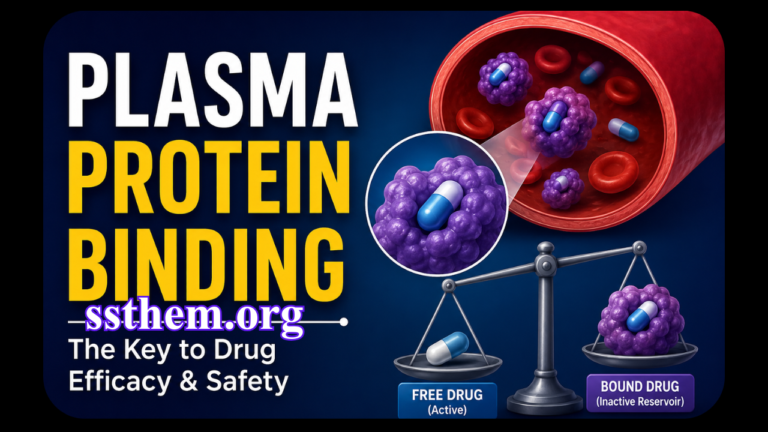
- Surrogate marker limitations: Plasma concentration is a surrogate measure for drug at the site of action
- Protein binding considerations: Highly protein-bound drugs may have high total plasma concentrations but low concentrations of free (active) drug
- Bioavailability may exceed 1.0: Recent research has challenged the conventional assumption that bioavailability cannot exceed 1.0
20. Common Misconceptions
Misconception 1: Bioavailability equals absorption
Reality: Absorption is the process of drug entering the bloodstream; bioavailability accounts for losses during this process, including first-pass metabolism.
Misconception 2: Higher bioavailability is always better
Reality: For some drugs, excessive bioavailability may increase toxicity risk. The goal is achieving predictable, consistent bioavailability within the therapeutic window.
Misconception 3: Generic drugs have lower bioavailability
Reality: Regulatory standards require bioequivalence for generic drugs. Studies demonstrate that bioequivalent products produce equivalent plasma concentrations and therapeutic effects.
Misconception 4: Oral bioavailability is the only consideration
Reality: While oral bioavailability receives significant attention, other routes (sublingual, buccal, rectal) may provide advantages in specific clinical scenarios.
Misconception 5: Food always reduces bioavailability
Reality: Food can increase bioavailability by enhancing dissolution, reducing stomach acid degradation, or inhibiting efflux transporters. Food effects are drug-specific.
Misconception 6: Bioavailability cannot exceed 100%
Reality: Studies have demonstrated that bioavailability determined using systemic concentration AUC measurements can exceed 1.0. While it is generally believed that bioavailability cannot exceed 1.0, research using Kirchhoff’s Laws has shown that AUC reflects not only systemic elimination but also absorption rate characteristics. Importantly, these findings do not impact regulatory guidance.
21. Recent Clinical Research
Current Knowledge on Bioavailability
Recent research published in The AAPS Journal (2024) challenged conventional understanding of bioavailability measurement. Using Kirchhoff’s Laws, researchers demonstrated that bioavailability determined using systemic concentration measurements may be overestimated for many drugs since AUC reflects not only systemic elimination but also absorption rate characteristics. This insight has significant implications for interpreting bioavailability data but does not affect regulatory guidance for bioequivalence testing.
Emerging Research Areas
Nanoparticle Formulations: Nanotechnology approaches aim to enhance solubility and absorption of poorly bioavailable drugs. Research demonstrates that 90% of new chemical entities are insufficiently water-soluble.
Physiologically-Based Pharmacokinetic (PBPK) Modeling: PBPK models integrate in vitro data to provide in vivo context, enabling predictions of drug-drug interactions, pharmacokinetic profiles, and population variability.
Self-Emulsifying Drug Delivery Systems (SEDDS): The development of multifunctional systems capable of combining controlled release, targeted delivery, and diagnostic capabilities is a promising avenue.
Macromolecular Drug Delivery: Research focuses on overcoming absorption barriers for macromolecular drugs through oral, transdermal, mucosal, and ocular delivery systems.
Question 1: What is bioavailability in pharmacology? (فارماکولوجی میں بائیو دستیابی کیا ہے؟)
Question 2: What is the difference between bioavailability and bioequivalence? (بائیو دستیابی اور بائیو ایکویولینس میں کیا فرق ہے؟)
Question 3: How is bioavailability measured? (بائیو دستیابی کی پیمائش کیسے کی جاتی ہے؟)
Question 4: What is the bioavailability formula? (بائیو دستیابی کا فارمولا کیا ہے؟)
Question 5: What is absolute bioavailability? (مطلق بائیو دستیابی کیا ہے؟)
Question 6: What is relative bioavailability? (نسبتی بائیو دستیابی کیا ہے؟)
Question 7: What factors affect drug bioavailability? (دوائیوں کی بائیو دستیابی کو کون سے عوامل متاثر کرتے ہیں؟)
Question 8: What is first-pass metabolism? (فرسٹ پاس میٹابولزم کیا ہے؟)
Question 9: What is the difference between oral and IV bioavailability? (زبانی اور نس بائیو دستیابی میں کیا فرق ہے؟)
Question 10: What is bioequivalence? (بائیو ایکویولینس کیا ہے؟)
Question 11: What is the bioavailability of IV drugs? (نس کے ذریعے دی جانے والی دوائیوں کی بائیو دستیابی کیا ہے؟)
Question 12: What drugs have high bioavailability? (کن دوائیوں کی بائیو دستیابی زیادہ ہوتی ہے؟)
Question 13: What drugs have low bioavailability? (کن دوائیوں کی بائیو دستیابی کم ہوتی ہے؟)
Question 14: What is AUC in bioavailability? (بائیو دستیابی میں AUC کیا ہے؟)
Question 15: How does first-pass effect affect bioavailability? (فرسٹ پاس اثر بائیو دستیابی کو کیسے متاثر کرتا ہے؟)
Question 16: Why is bioavailability important? (بائیو دستیابی کیوں اہم ہے؟)
Question 17: How do disease states affect bioavailability? (بیماریاں بائیو دستیابی کو کیسے متاثر کرتی ہیں؟)
Question 18: What is the role of bioavailability in generic drug approval? (جنرک دوائیوں کی منظوری میں بائیو دستیابی کا کیا کردار ہے؟)
Question 19: What is plasma protein binding and how does it affect bioavailability? (پلازما پروٹین بائنڈنگ کیا ہے اور یہ بائیو دستیابی کو کیسے متاثر کرتی ہے؟)
Question 20: What is the role of transporters in bioavailability? (بائیو دستیابی میں ٹرانسپورٹرز کا کیا کردار ہے؟)
Question 21: How do genetic factors affect bioavailability? (جینیاتی عوامل بائیو دستیابی کو کیسے متاثر کرتے ہیں؟)
Question 22: What is the clinical significance of bioavailability? (بائیو دستیابی کی طبی اہمیت کیا ہے؟)
Question 23: How is bioavailability measured in clinical practice? (کلینیکل پریکٹس میں بائیو دستیابی کی پیمائش کیسے کی جاتی ہے؟)
Question 24: What is the role of bioavailability in drug safety? (دوائی کی حفاظت میں بائیو دستیابی کا کیا کردار ہے؟)
Question 25: How does absorption affect bioavailability? (جذب بائیو دستیابی کو کیسے متاثر کرتا ہے؟)
Question 26: What are the types of bioavailability? (بائیو دستیابی کی اقسام کیا ہیں؟)
Question 27: How do disease conditions affect bioavailability? (بیماریاں بائیو دستیابی کو کیسے متاثر کرتی ہیں؟)
Question 28: What is the bioavailability concept in pharmacology? (فارماکولوجی میں بائیو دستیابی کا تصور کیا ہے؟)
Question 29: How does route of administration affect bioavailability? (استعمال کا راستہ بائیو دستیابی کو کیسے متاثر کرتا ہے؟)
Question 30: What is the difference between absolute and relative bioavailability? (مطلق اور نسبتی بائیو دستیابی میں کیا فرق ہے؟)
23. Key Takeaways
- Definition: Bioavailability is the fraction of administered drug dose that reaches systemic circulation unchanged, representing both rate and extent of absorption.
- IV is the gold standard: Intravenous administration provides 100% bioavailability, serving as the reference for all other routes.
- Absolute vs. Relative: Absolute bioavailability compares non-IV to IV; relative bioavailability compares two non-IV formulations.
- First-pass metabolism is critical: This presystemic metabolism in the gut and liver significantly reduces oral bioavailability.
- AUC is the key measure: The area under the plasma concentration–time curve is the most reliable measure of bioavailability.
- Multiple factors influence bioavailability: Drug formulation, patient physiology, disease states, genetics, and drug–drug interactions all play roles.
- Bioequivalence ensures consistency: Generic drugs must demonstrate bioequivalence to branded products.
- Clinical relevance: Bioavailability determines dosing, guides route selection, and influences therapeutic outcomes.
- Special populations require attention: Children, pregnant women, and elderly patients may have altered bioavailability requiring dose adjustments.
- Personalized medicine advances: Understanding bioavailability facilitates individualized therapy and optimized drug delivery.
- Bioavailability enhancement: Over 90% of pharmaceuticals have limitations on oral bioavailability, driving research into novel strategies.
- Emerging technologies: Self-emulsifying drug delivery systems, nanotechnology, and PBPK modeling represent the future of bioavailability optimization.
24. References
Major Pharmacology Textbooks
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics. 13th Edition. New York: McGraw-Hill.
- Katzung BG, Vanderah TW. Basic & Clinical Pharmacology. 15th Edition. New York: McGraw-Hill.
- Rang HP, Dale MM, Ritter JM, Flower RJ, Henderson G. Rang & Dale’s Pharmacology. 9th Edition. Elsevier.
Regulatory and Clinical References
- FDA. M9 Biopharmaceutics Classification System-Based Biowaivers. Guidance Document. May 2021.
- FDA. Bioavailability Studies Submitted in NDAs or INDs – General Considerations. Guidance Document. 2022.
- FDA. Bioavailability and Bioequivalence Requirements. 21 CFR Part 320.
- EMA. Guidelines on the investigation of bioequivalence.
- WHO. Bioavailability and Bioequivalence Studies. World Health Organization.
Peer-Reviewed Literature
- Almukainzi M, et al. Drug Absorption. In: StatPearls. Treasure Island (FL): StatPearls Publishing. 2024.
- Wakuda H, Xiang Y, Sodhi JK, Uemura N, Benet LZ. An Explanation of Why Dose-Corrected Area Under the Curve for Alternate Administration Routes Can Be Greater than for Intravenous Dosing. The AAPS Journal. 2024;26(1).
- Dash JR, et al. Novel Approaches for the Enhancement of Bioavailability of Drugs: An Updated Review. Curr Drug Discov Technol. 2025;22(4).
- Pond SM, et al. First-pass elimination. Basic concepts and clinical consequences. Clin Pharmacokinet. 1984 Jan-Feb;9(1):1-25.
- Al-Amiry Santos LG, Polak S, Rowland Yeo K. Evaluating the Impact of Intestinal Bile Salts on Drug Absorption Using PBPK Modeling. CPT Pharmacometrics Syst Pharmacol. 2026.
- Ritschel WA, et al. Evaluation of bioavailability by different methods. Methods Find Exp Clin Pharmacol. 1985 Aug;7(8):439-49.
Additional Resources
- British National Formulary (BNF). Provides prescribing information and guidance on drug administration.
- EUPATI Open Classroom. Bioavailability and Bioequivalence studies.
- Merck Manual. Drug Bioavailability. Professional Edition.
Bioavailability is a fundamental concept in pharmacology that underpins the entire field of pharmacotherapy. Understanding the mechanisms, factors, and clinical implications of bioavailability is essential for healthcare professionals to optimize drug therapy and improve patient outcomes.
From the simple diffusion of lipid-soluble molecules across cell membranes to the complex interplay of transporters, enzymes, and physiological factors, bioavailability represents a remarkable example of the intricate relationship between drugs and the human body.
Remember: The success of pharmacotherapy depends not only on the pharmacological properties of the drug but also on its ability to reach the site of action in adequate concentrations. A thorough understanding of bioavailability principles empowers clinicians to make informed decisions about drug selection, dosing, and route of administration.
As research continues to advance our understanding of bioavailability through PBPK modeling, nanotechnology, and personalized medicine approaches, the future holds promise for more effective and tailored drug therapy for all patients.
Disclaimer (ڈس کلیمر): یہ تعلیمی مواد صرف معلوماتی مقاصد کے لیے تیار کیا گیا ہے تاکہ فارماکولوجی میں بائیو دستیابی (Bioavailability) کے بارے میں سمجھ بوجھ بڑھائی جا سکے۔ یہ کسی بھی قسم کی طبی مشاورت، تشخیص یا علاج کا متبادل نہیں ہے۔ کسی بھی دوائی کا استعمال کرنے سے پہلے ہمیشہ کسی مستند معالج یا فارماسسٹ سے مشورہ کریں۔ اس مضمون میں دی گئی معلومات تازہ ترین سائنسی تحقیقات اور مستند طبی حوالوں پر مبنی ہے تاہم ادویات کے استعمال سے متعلق کوئی بھی فیصلہ کرنے سے پہلے اپنے معالج سے ضرور مشورہ کریں۔
آخری اپ ڈیٹ: جولائی 2026 | ورژن: 2.0 | نظرثانی کی مدت: سالانہ نظرثانی تجویز کردہ
This educational content is for informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always consult your physician or pharmacist before taking any medication.