First-Pass Effect in First-Pass Metabolism 7 Powerful Insights Every Clinician Must Know
First-Pass Effect (First-Pass Metabolism) Complete Evidence-Based Guide (2026)
The first-pass effect—also called first-pass metabolism or presystemic metabolism—is a fundamental pharmacological phenomenon that significantly influences drug therapy outcomes. When a medication is administered orally, it must navigate the gastrointestinal tract, intestinal wall, and liver before reaching systemic circulation. Along this pathway, drug-metabolising enzymes can reduce the concentration of the active compound, sometimes eliminating over 90 % of the administered dose.
Understanding this process is critical for appropriate dosing, route selection, and anticipating drug interactions. The first-pass effect represents one of the most clinically important concepts in pharmacokinetics, directly impacting bioavailability, therapeutic efficacy, and patient safety. This evidence-based guide synthesises current pharmacological knowledge to provide a thorough understanding of this phenomenon.
Want to explore authentic information about the world’s religions, beliefs, and history? Visit ssthem.com today!
Table of Contents
- 1. Definition of the First‑Pass Effect
- 2. Historical Background
- 3. How the First‑Pass Effect Occurs
- 4. Role of the Liver
- 5. Role of the Small Intestine
- 6. Cytochrome P450 (CYP450) Enzymes
- 7. How First‑Pass Reduces Bioavailability
- 8. Clinical Importance
- 9. Drugs with Significant First‑Pass Effect
- 10. Drugs with Minimal First‑Pass Effect
- 11. Routes That Bypass First‑Pass
- 12. Factors Influencing First‑Pass
- 13. Pharmacokinetic Models
- 14. Clinical Examples
- 15. Advantages & Disadvantages
- 16. Strategies to Overcome First‑Pass
- 17. Differences: Bioavailability & Clearance
- 18. Common Misconceptions
- 19. Current Research & Evidence
- 20. Frequently Asked Questions
- 21. Key Takeaways
- 22. References
1. Definition of the First‑Pass Effect
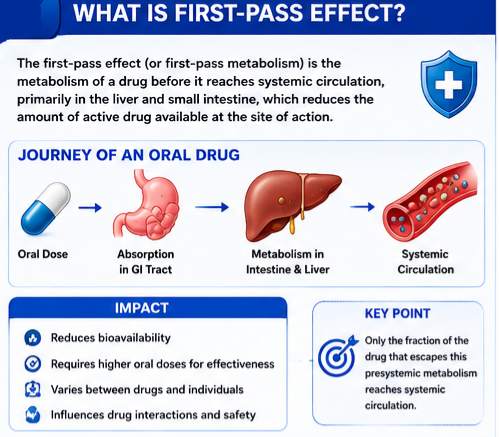 The first‑pass effect is a pharmacological phenomenon in which a medication undergoes metabolism at specific locations in the body before reaching systemic circulation or its site of action. This metabolic processing reduces the concentration of the active drug available to produce its therapeutic effect.
The first‑pass effect is a pharmacological phenomenon in which a medication undergoes metabolism at specific locations in the body before reaching systemic circulation or its site of action. This metabolic processing reduces the concentration of the active drug available to produce its therapeutic effect.
More precisely, the first‑pass effect refers to the biotransformation of a drug before it enters the systemic circulation, with the most significant effects typically occurring in the liver and small intestine. The term “presystemic metabolism” is often used interchangeably, reflecting that metabolism occurs before the drug reaches the systemic circulation.
The clinical importance of this phenomenon cannot be overstated. When a drug undergoes extensive first‑pass metabolism, oral administration requires significantly higher doses to achieve therapeutic concentrations compared to intravenous administration. In some cases, the first‑pass effect is so pronounced that oral administration becomes impractical or impossible.
2. First-Pass Effect Historical Background
The recognition of the first‑pass effect emerged as pharmacokinetics developed as a scientific discipline in the mid‑20th century. Early pharmacologists observed that certain drugs required substantially higher oral doses compared to intravenous doses to achieve comparable effects. This observation led to systematic investigation of metabolic barriers between drug administration and systemic circulation.
The 1970s and 1980s saw significant advances in understanding the mechanisms underlying first‑pass metabolism. Researchers identified the liver as the primary site of this effect and began characterising the specific enzymes responsible for drug metabolism. The discovery of the cytochrome P450 enzyme system and its role in first‑pass metabolism represented a major breakthrough.
More recently, recognition that the gastrointestinal tract itself contributes substantially to first‑pass metabolism has refined our understanding. The discovery of high concentrations of CYP3A4 and CYP2D6 in the intestinal brush border transformed the first‑pass effect from a primarily hepatic phenomenon to one with significant intestinal components.
3. How the First‑Pass Effect Occurs
 The journey of an orally administered drug through the body involves several sequential stages where metabolism can occur. Understanding these stages is essential for predicting and managing the first‑pass effect.
The journey of an orally administered drug through the body involves several sequential stages where metabolism can occur. Understanding these stages is essential for predicting and managing the first‑pass effect.
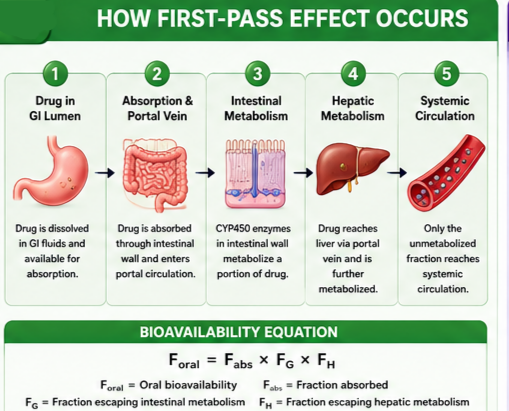
3.1 Drug Absorption from the Gastrointestinal Tract
Following oral administration, the drug must first dissolve in gastrointestinal fluids and then cross the intestinal epithelium. During this process, multiple barriers can reduce the amount of active drug available:
- Chemical degradation: Gastric acid and digestive enzymes may break down certain drugs before absorption.
- Incomplete absorption: Not all of the administered dose may cross the intestinal membrane.
- Active export: Transport proteins like P‑glycoprotein can pump drugs back into the intestinal lumen.
The extent of absorption varies considerably among drugs based on their physicochemical properties (lipophilicity, molecular size, ionisation state).
3.2 Portal Venous Circulation
Drugs absorbed from the gastrointestinal tract enter the portal venous system, which directs blood flow from the intestines to the liver. This anatomical arrangement ensures that all substances absorbed from the gut—including nutrients, toxins, and drugs—pass through the liver before reaching the rest of the body.
3.3 Intestinal Metabolism
Historically, first‑pass metabolism was mainly attributed to the liver. However, important cytochrome P450 isozymes—particularly CYP3A4 and CYP2D6—are present at high concentrations in the intestinal brush border. The small intestine has a much larger surface area and lower blood flow than the liver, which further adds to the significance of intestinal first‑pass metabolism.
3.4 Hepatic Metabolism
The liver represents the most significant site of first‑pass metabolism. After passing through the intestinal wall, drugs enter the liver via the portal vein. Hepatic enzymes can extensively metabolise the drug before it reaches systemic circulation. The liver’s high capacity for extraction and biotransformation means it may efficiently limit the availability of drugs to other body sites.
3.5 Systemic Circulation
Only the fraction of the drug that survives intestinal and hepatic metabolism reaches the systemic circulation. This remaining portion is then distributed to target tissues where it can produce its therapeutic effects.
The amount of drug reaching systemic circulation can be expressed mathematically as:
Foral = Fabs × FG × FH
Where Foral = oral bioavailability, Fabs = fraction absorbed, FG = fraction passing the GI tract unmetabolised, and FH = hepatic first‑pass availability.
4. Role of the Liver
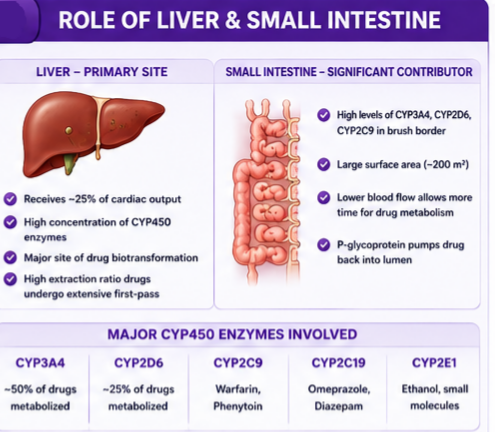 The liver serves as the primary site of first‑pass metabolism due to several anatomical and physiological features:
The liver serves as the primary site of first‑pass metabolism due to several anatomical and physiological features:
- Anatomical positioning: The liver receives blood from the gastrointestinal tract through the portal vein, ensuring that all orally absorbed substances encounter hepatic enzymes before reaching systemic circulation.
- High enzyme concentration: The liver contains the highest concentration of drug‑metabolising enzymes in the body, particularly cytochrome P450 enzymes.
- High blood flow: With approximately 25 % of cardiac output directed to the liver, this organ processes large volumes of blood.
- Multiple metabolic pathways: The liver possesses numerous enzyme systems capable of metabolising diverse chemical structures.
The hepatic extraction ratio—the fraction of drug removed from blood during a single pass through the liver—determines the extent of hepatic first‑pass metabolism. Drugs with high extraction ratios (>0.7) undergo extensive first‑pass metabolism, while those with low extraction ratios (<0.3) are minimally affected.
5. Role of the Small Intestine
The intestinal contribution to first‑pass metabolism has received increasing recognition in recent decades. The intestinal wall contains significant concentrations of drug‑metabolising enzymes that can substantially reduce drug bioavailability before hepatic metabolism occurs.
- Enzyme distribution: Important cytochrome P450 isozymes—particularly CYP3A4, CYP2D6, and CYP2C9—are present at high concentrations in the intestinal brush border.
- Surface area: The small intestine has an enormous surface area (approximately 200 m²), maximising contact between drugs and metabolising enzymes.
- Lower blood flow: The small intestine has lower blood flow relative to its surface area compared to the liver. This means metabolised drug may remain in the intestinal tissues longer, allowing more extensive metabolism.
- P‑glycoprotein activity: This efflux transporter can pump drugs back into the intestinal lumen, reducing absorption and effectively decreasing bioavailability.
6. First-Pass Effect Cytochrome P450 (CYP450) Enzymes
The cytochrome P450 enzyme superfamily plays a central role in first‑pass metabolism. These heme‑containing enzymes catalyse oxidative reactions that are fundamental to Phase I drug metabolism.
- CYP3A4: The most abundant CYP450 enzyme in the liver and intestine, responsible for metabolising approximately 50 % of all drugs. Substrates include cyclosporine, estradiol, and many protease inhibitors.
- CYP2D6: Responsible for metabolising approximately 25 % of drugs; shows considerable genetic polymorphism.
- CYP2C9: Important for metabolising drugs such as warfarin and phenytoin.
- CYP2C19: Metabolises drugs including omeprazole and diazepam.
The activity of CYP450 enzymes can be influenced by genetic polymorphisms, enzyme induction, enzyme inhibition, and dietary factors (e.g., grapefruit juice inhibits intestinal CYP3A4).
7. How the First‑Pass Effect Reduces Bioavailability
Bioavailability—the fraction of administered drug reaching systemic circulation—is the key measure affected by first‑pass metabolism. Experimentally, bioavailability is measured by comparing the Area‑Under‑the‑Curve (AUC) following oral administration to that following intravenous injection (which by definition produces 100 % bioavailability).
When first‑pass metabolism is significant, drugs must be given at higher oral doses to achieve therapeutic concentrations. For example:
- Propranolol has approximately 26 % oral bioavailability because 75–85 % is metabolised before reaching systemic circulation.
- Morphine has approximately 30 % oral bioavailability because 70 % undergoes first‑pass metabolism.
- Lidocaine has such extensive first‑pass metabolism (3 % oral bioavailability) that it is not used orally.
8. Clinical Importance
The clinical significance of the first‑pass effect extends to multiple aspects of pharmacological therapy:
- Dosing considerations: Drugs undergoing significant first‑pass metabolism require oral dosages much larger than intravenous dosages.
- Route selection: When first‑pass metabolism is extensive, alternative administration routes may be necessary (e.g., nitroglycerin, lidocaine, naloxone are typically not given orally).
- Monitoring considerations: Monitoring blood concentrations of drugs subject to the first‑pass effect is the most viable way to maintain therapeutic concentrations, especially for drugs with narrow therapeutic windows.
- Individual variability: Many enzymes involved in first‑pass metabolism are subject to genetic variability, leading to differences in drug response among patients.
- Drug interactions: Drugs subject to first‑pass metabolism are prone to more drug interactions at the metabolic level.
9. Drugs with Significant First‑Pass Effect
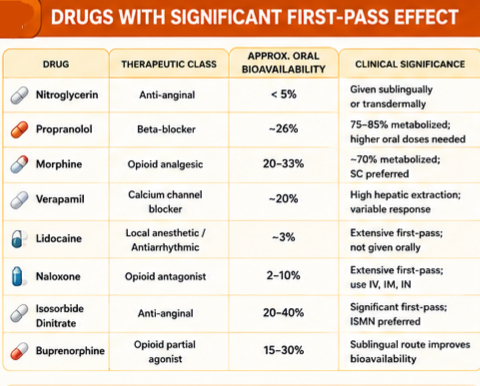 Additional drugs: Alprenolol, amitriptyline, 5‑fluorouracil, hydralazine, isoprenaline, lorcainide, pethidine, mercaptopurine, metoprolol, neostigmine, nifedipine, pentazocine.
Additional drugs: Alprenolol, amitriptyline, 5‑fluorouracil, hydralazine, isoprenaline, lorcainide, pethidine, mercaptopurine, metoprolol, neostigmine, nifedipine, pentazocine.
10. Drugs with Minimal First‑Pass Effect
- Levofloxacin: Oral bioavailability > 99 %; allows direct IV‑to‑oral switch.
- Digoxin: Limited first‑pass; 60‑80 % bioavailability.
- Amoxicillin: 70‑90 % bioavailability; minimal first‑pass.
- Gabapentin: ~60 % bioavailability; minimal first‑pass.
- Phenytoin: Variable but good oral bioavailability; low hepatic extraction.
- Warfarin: Near‑complete absorption; minimal first‑pass effect.
11. Routes That Bypass the First‑Pass Effect
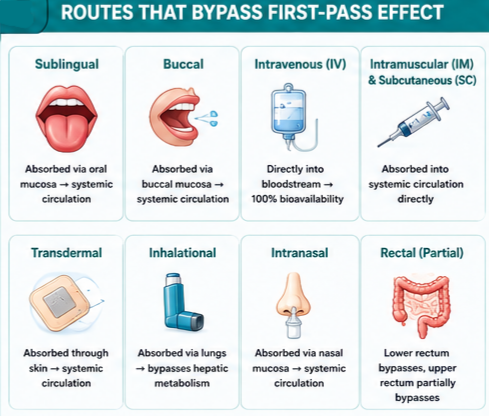
- Sublingual: Absorbed through oral mucosa → systemic circulation (e.g., nitroglycerin).
- Buccal: Similar to sublingual; bypasses hepatic metabolism.
- Intravenous (IV): Directly into bloodstream → 100 % bioavailability.
- Intramuscular (IM) / Subcutaneous (SC): Bypass hepatic first‑pass.
- Transdermal: Absorbed through skin → systemic circulation.
- Inhalational: Absorbed through lungs; bypasses hepatic metabolism (though pulmonary metabolism may occur).
- Intranasal: Absorbed through nasal mucosa → systemic circulation.
- Rectal: Partial bypass; lower rectum drains directly into systemic circulation, but upper rectum and colon drain into portal circulation.
12. Factors Influencing the First‑Pass Effect
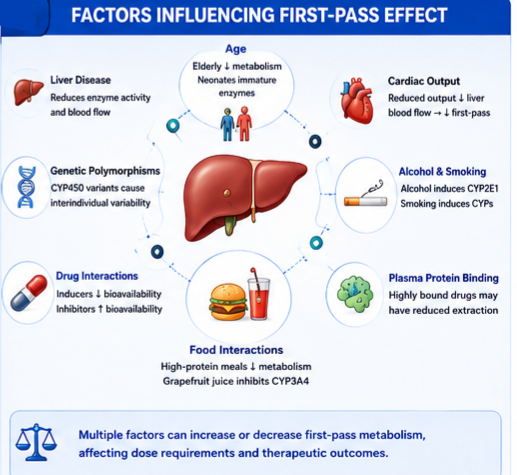
- Liver disease: Reduces enzyme activity and blood flow → decreased first‑pass → increased bioavailability.
- Age: Elderly have reduced liver blood flow and mass; neonates have immature enzyme systems.
- Gender: Differences in first‑pass effect noted between males and females.
- Cardiac output: Reduced output decreases hepatic blood flow → reduced first‑pass.
- Genetic polymorphisms: CYP450 variants create interindividual differences (poor metabolisers vs. ultra‑rapid metabolisers).
- CYP450 induction/inhibition: Rifampin (inducer) reduces bioavailability; cimetidine (inhibitor) increases bioavailability.
- Food interactions: High‑protein meals may inhibit metabolism; grapefruit juice inhibits intestinal CYP3A4.
- Alcohol & smoking: Chronic alcohol induces CYP2E1; smoking induces certain CYP450 enzymes.
- Plasma protein binding: Highly bound drugs may have reduced hepatic extraction.
13. Pharmacokinetic Models of First‑Pass Metabolism
Two widely applied models describe the dependence of bioavailability on changes in physiological variables for drugs subject to first‑pass metabolism only in the liver:
- The ‘Well‑Stirred’ Model: Assumes the liver is a well‑stirred compartment where drug concentration in the liver equals that in the outflowing blood. Changes in enzyme activity, blood flow, or protein binding have a relatively moderate effect on bioavailability.
- The ‘Parallel Tube’ Model: Assumes the liver consists of parallel tubes where drug concentration decreases exponentially. This model predicts a much greater change in bioavailability for a given change in enzyme activity, blood flow, or unbound fraction.
The predictions of the models are similar when bioavailability is large but differ dramatically when bioavailability is small.
14. Clinical Examples
Nitroglycerin in Angina
Oral nitroglycerin undergoes extensive first‑pass metabolism, rendering it ineffective for acute angina. Sublingual nitroglycerin bypasses first‑pass and relieves symptoms within 2 minutes. For chronic management, transdermal patches provide sustained delivery.
Morphine Oral vs. Intravenous Dosing
Approximately 70 % of oral morphine is metabolised during first‑pass (bioavailability ~30 %). A 10 mg IV dose may provide equivalent effect to 30‑40 mg oral dose. Morphine is often given subcutaneously for rapid, predictable analgesia.
Naloxone and Oral Administration
Naloxone has 2‑10 % oral bioavailability due to extensive presystemic metabolism. It is administered IV, IM, or intranasally for acute opioid reversal. In some contexts, oral naloxone is used for opioid‑induced constipation, where systemic absorption is undesirable.
Verapamil Bioavailability
Verapamil has approximately 20 % oral bioavailability due to extensive hepatic first‑pass. Oral doses must be significantly higher than IV doses, and individual variability in hepatic metabolism contributes to variable responses.
Dextromethorphan + Quinidine
Dextromethorphan (substrate for CYP2D6) undergoes significant first‑pass bioinactivation. Coadministration with a low dose of quinidine inhibits first‑pass metabolism, increasing systemic concentrations. This combination is FDA‑approved for pseudobulbar affect.
15. Advantages & Disadvantages of the First‑Pass Effect
Advantages
- Protection against toxins: Detoxifies xenobiotics that would otherwise accumulate.
- Oral tolerance: May prevent overreaction to dietary antigens.
- Local drug activity: Limits systemic exposure for drugs acting locally in the GI tract (e.g., orlistat).
- Reduced systemic accumulation: Limits active drug reaching systemic circulation, reducing toxicity risk.
- Therapeutic advantage: Budesonide inhalation uses first‑pass to reduce systemic bioavailability and minimise adverse effects.
Disadvantages
- Reduced bioavailability: Requires higher oral doses, making therapy inefficient or economically disadvantageous.
- Individual variability: Genetic polymorphisms create significant interpatient variation.
- Drug interactions: Inhibition or induction of CYP450 can produce unpredictable effects.
- High interpatient variability: Makes dosing challenging, especially for drugs with narrow therapeutic windows.
- Metabolite effects: First‑pass metabolites may have different (sometimes toxic) pharmacological activities.
- Variable food effects: Food can unpredictably affect first‑pass metabolism, complicating dosing and patient counselling.
16. Strategies to Overcome First‑Pass Metabolism
- Enzyme inhibition: Coadminister with an inhibitor to boost bioavailability (e.g., cyclosporine + ketoconazole; dextromethorphan + quinidine; lopinavir + ritonavir).
- Lipid‑based formulations: Very lipophilic compounds (log10P 5‑6) may enter systemic circulation via the lymphatic pathway, bypassing first‑pass.
- Novel drug delivery systems: Self‑microemulsifying drug delivery systems (SMEDDS), microemulsions, solid lipid nanoparticles.
- Prodrug approach: Prodrugs can protect drugs from rapid first‑pass metabolism (e.g., bambuterol prodrug of terbutaline).
17. Differences: First‑Pass Effect vs. Bioavailability & Clearance
First‑Pass Effect vs. Bioavailability
- First‑pass effect: The metabolic processing that occurs before a drug reaches systemic circulation.
- Bioavailability: The fraction of administered drug that reaches systemic circulation unchanged.
- Relationship: The first‑pass effect is one component (often the most significant) that determines bioavailability.
First‑Pass Effect vs. Drug Clearance
- First‑pass effect: Presystemic metabolism during absorption phase.
- Drug clearance: Volume of blood from which drug is completely removed per unit time; occurs throughout the drug’s presence in the body.
- Key distinction: First‑pass primarily affects bioavailability; clearance affects steady‑state concentrations and dosing intervals.
18. Common Misconceptions
- Misconception: First‑pass effect occurs only in the liver.
Reality: The intestine, blood, vascular endothelium, lungs, and even the arm from which venous samples are taken can contribute. - Misconception: Intravenous drugs do not undergo first‑pass metabolism.
Reality: IV bypasses intestinal and hepatic first‑pass, but pulmonary first‑pass and metabolism in blood/vascular endothelium may still occur. - Misconception: Rectal administration completely bypasses first‑pass.
Reality: Only a portion of rectally administered drug bypasses the portal circulation; the upper rectum and colon drain into portal circulation. - Misconception: Higher oral doses simply overcome first‑pass metabolism.
Reality: Increasing doses also increases metabolite production and may cause toxicity; enzymatic saturation can alter bioavailability unpredictably. - Misconception: First‑pass effect is the same for all patients.
Reality: Genetic polymorphisms, liver function, age, gender, and concomitant medications create substantial variability.
19. Current Research & Clinical Evidence
- Intestinal Metabolism: Recent discoveries of high CYP450 concentrations in the intestinal brush border have transformed understanding of first‑pass metabolism.
- Drug‑Drug Interaction Studies: Cyclosporine bioavailability boosted by ketoconazole (CYP3A4 inhibitor); dextromethorphan + quinidine for pseudobulbar affect.
- Lipid‑Based Formulations: Very lipophilic compounds (log10P 5‑6) may enter systemic circulation via the lymphatic pathway, bypassing first‑pass.
- Food‑Effect Research: High‑protein meals may temporarily inhibit drug metabolism in addition to increasing liver blood flow.
- Genetic Variability: Polymorphisms in CYP450 enzymes contribute to interindividual differences in drug response.
- Clinical Guidelines: Major pharmacology textbooks (Goodman & Gilman’s, Katzung & Trevor’s, Rang & Dale’s) provide evidence‑based guidance.
21. Key Takeaways
- Definition and mechanism: The first‑pass effect is presystemic metabolism that reduces drug concentration before reaching systemic circulation, primarily occurring in the liver and small intestine.
- Clinical importance: Understanding the first‑pass effect is crucial for proper dosing, route selection, drug interaction management, and anticipating individual variability in drug response.
- Bioavailability impact: First‑pass metabolism significantly reduces oral bioavailability, requiring higher oral doses compared to IV doses for drugs with extensive presystemic metabolism.
- Multiple sites of metabolism: While the liver is the primary site, the small intestine contributes substantially through CYP3A4, CYP2D6, and other enzymes. Other sites include blood, vascular endothelium, and lungs.
- Alternative routes: Sublingual, buccal, IV, IM, SC, transdermal, inhalational, intranasal, and rectal (partial) administration bypass hepatic first‑pass metabolism.
- Drugs with significant effect: Major examples include nitroglycerin, propranolol, morphine, verapamil, lidocaine, and naloxone.
- Factors influencing effect: Liver disease, age, gender, cardiac output, genetic polymorphisms, CYP450 induction/inhibition, food interactions, and alcohol/smoking all affect first‑pass metabolism.
- Drug interactions: Drug‑drug interactions at CYP450 enzymes can significantly alter the bioavailability of drugs subject to first‑pass metabolism.
- Clinical monitoring: Therapeutic drug monitoring is valuable for drugs subject to first‑pass metabolism, particularly those with narrow therapeutic windows.
- Patient variability: Genetic polymorphisms in metabolising enzymes contribute to significant interindividual variation in drug response.
22. References
Major Pharmacology Textbooks
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics. 13th Edition. New York: McGraw‑Hill.
- Katzung BG, Vanderah TW. Basic & Clinical Pharmacology. 15th Edition. New York: McGraw‑Hill.
- Rang HP, Dale MM, Ritter JM, Flower RJ, Henderson G. Rang & Dale’s Pharmacology. 9th Edition. Elsevier.
Regulatory & Clinical References
- FDA. M9 Biopharmaceutics Classification System‑Based Biowaivers. Guidance Document. May 2021.
- FDA. Bioavailability Studies Submitted in NDAs or INDs – General Considerations. Guidance Document. 2022.
- EMA. Guidelines on the investigation of bioequivalence.
- WHO. Bioavailability and Bioequivalence Studies.
Peer‑Reviewed Literature
- Pond SM, et al. First‑pass elimination. Basic concepts and clinical consequences. Clin Pharmacokinet. 1984 Jan‑Feb;9(1):1‑25.
- Wakuda H, Xiang Y, Sodhi JK, Uemura N, Benet LZ. An Explanation of Why Dose‑Corrected Area Under the Curve for Alternate Administration Routes Can Be Greater than for Intravenous Dosing. The AAPS Journal. 2024;26(1).
- Dash JR, et al. Novel Approaches for the Enhancement of Bioavailability of Drugs: An Updated Review. Curr Drug Discov Technol. 2025;22(4).
- Al‑Amiry Santos LG, Polak S, Rowland Yeo K. Evaluating the Impact of Intestinal Bile Salts on Drug Absorption Using PBPK Modeling. CPT Pharmacometrics Syst Pharmacol. 2026.
Disclaimer (ڈس کلیمر): یہ تعلیمی مواد صرف معلوماتی مقاصد کے لیے تیار کیا گیا ہے تاکہ فارماکولوجی میں فرسٹ پاس اثر (First‑Pass Effect) کے بارے میں سمجھ بوجھ بڑھائی جا سکے۔ یہ کسی بھی قسم کی طبی مشاورت، تشخیص یا علاج کا متبادل نہیں ہے۔ کسی بھی دوائی کا استعمال کرنے سے پہلے ہمیشہ کسی مستند معالج یا فارماسسٹ سے مشورہ کریں۔ اس مضمون میں دی گئی معلومات تازہ ترین سائنسی تحقیقات اور مستند طبی حوالوں پر مبنی ہے تاہم ادویات کے استعمال سے متعلق کوئی بھی فیصلہ کرنے سے پہلے اپنے معالج سے ضرور مشورہ کریں۔
آخری اپ ڈیٹ: جولائی 2026 | ورژن: 2.0 | نظرثانی کی مدت: سالانہ نظرثانی تجویز کردہ
This educational content is for informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always consult your physician or pharmacist before taking any medication.
© 2026 · First‑Pass Effect Guide · All rights reserved.