5 Critical Drug Interactions You Must Know The Role of Plasma Protein Binding
Plasma Protein Binding in Clinical Pharmacology: From Molecular Mechanisms to Therapeutic Implications
Plasma protein binding (PPB) describes the reversible association between drugs and circulating proteins in the bloodstream. This interaction profoundly influences drug distribution, metabolism, excretion, and ultimately, therapeutic efficacy. While the pharmacological effect of a drug correlates most closely with its unbound (free) concentration at the site of action, routine clinical monitoring typically measures total drug concentration—a composite of both bound and free fractions.
The clinical relevance of PPB changes has been controversially discussed for decades. Some authors have argued that protein binding alterations are clinically insignificant for most drugs, while others contend that such changes can dramatically impact patient outcomes. Contemporary understanding recognizes that a generalized “one-size-fits-all” approach is inappropriate; instead, careful analysis of PPB effects must be conducted on a drug-by-drug basis, considering both pharmacokinetic and pharmacodynamic processes.
This article provides a comprehensive review of the theoretical concepts of plasma protein binding, the physiological characteristics of major binding proteins, mechanisms of drug-protein interaction, and the clinical significance of PPB alterations across various patient populations.
Table of Contents
- 1. Definition of Plasma Protein Binding
- 2. Historical Background
- 3. Importance in Clinical Pharmacology
- 4. Physiology of Plasma Proteins
- 5. Mechanism of Drug–Protein Binding
- 6. Bound vs. Free Drug Fraction
- 7. Factors Affecting Plasma Protein Binding
- 8. Highly Protein-Bound Drugs (Comparison Table)
- 9. Low Protein-Bound Drugs
- 10. Clinical Significance
- 11. Drug Interactions & Disease Impact
- 12. Measurement Methods
- 13. Clinical Case Examples
- 14. Therapeutic Drug Monitoring
- 15. Common Misconceptions
- 16. Frequently Asked Questions (FAQs)
- 17. Key Takeaways
- 18. References
1. Definition of Plasma Protein Binding
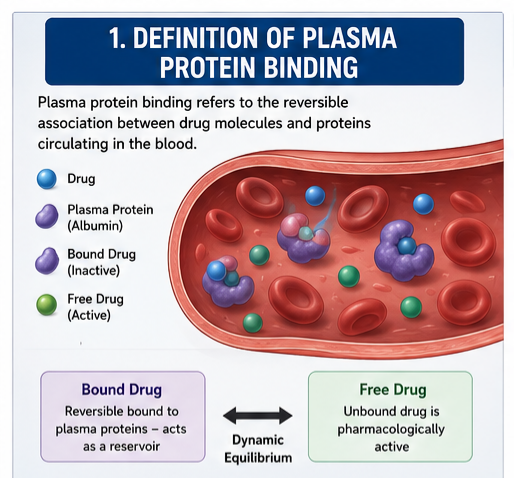 Plasma protein binding refers to the reversible association between drug molecules and proteins circulating in the blood. When a drug enters the bloodstream, it exists in two forms: a bound fraction, attached to plasma proteins, and an unbound (free) fraction, dissolved in plasma water. These two fractions exist in dynamic equilibrium, with the bound fraction serving as a circulating reservoir.
Plasma protein binding refers to the reversible association between drug molecules and proteins circulating in the blood. When a drug enters the bloodstream, it exists in two forms: a bound fraction, attached to plasma proteins, and an unbound (free) fraction, dissolved in plasma water. These two fractions exist in dynamic equilibrium, with the bound fraction serving as a circulating reservoir.
The extent of binding is typically expressed as the percentage of total drug that is protein-bound, or alternatively, as the fraction unbound (fu). Drugs are classified based on their binding affinity:
| Binding Category | Percentage Bound | Clinical Significance |
|---|---|---|
| Negligible | 0–50% | Changes in protein binding rarely clinically significant |
| Moderate | 50–90% | May require monitoring in certain conditions |
| High | 90–99% | Clinically significant changes possible |
| Very High | >99% | Even small changes in binding can produce large effects |
2. Historical Background
The recognition that drugs associate with blood components dates to the early 20th century. However, systematic investigation of drug-protein binding emerged in the 1960s and 1970s, driven by advances in analytical techniques and growing awareness that pharmacokinetic behaviour could not be fully understood without considering protein interactions. The discovery that warfarin—a drug with 99% protein binding—exhibited significant variability in its pharmacological response led to intensive investigation of binding phenomena.
Initially, binding to plasma proteins was considered primarily a storage mechanism, with bound drug serving as a reservoir that maintains free drug concentrations as the drug is eliminated. The clinical relevance of PPB became increasingly apparent as clinicians observed that conditions altering plasma protein concentrations—such as liver disease, renal impairment, and pregnancy—could significantly affect drug response and toxicity profiles.
The development of equilibrium dialysis methods in the 1970s enabled more precise quantification of binding parameters. The introduction of Rapid Equilibrium Dialysis (RED) devices represented a significant technological advancement, reducing equilibration times from 16–24 hours to 4–6 hours while maintaining accuracy and reproducibility.
3. Importance in Clinical Pharmacology
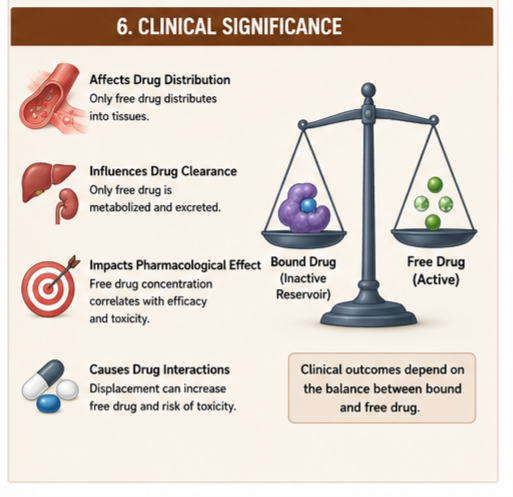
Plasma protein binding is a cornerstone of pharmacokinetic science. It influences:
- Drug distribution – only unbound drug leaves the vascular compartment
- Drug metabolism – only unbound drug is available for hepatic clearance
- Drug excretion – only unbound drug is filtered by the glomerulus
- Pharmacodynamic response – free drug concentration correlates with effect
- Drug-drug interactions – displacement from binding sites can alter free concentrations
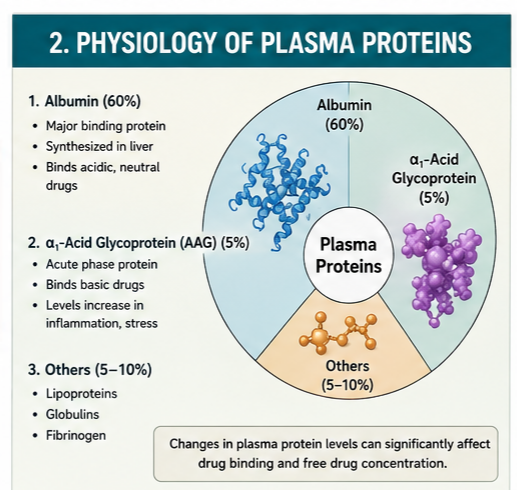
4. Physiology of Plasma Proteins
Human Serum Albumin (HSA)
Albumin is the most abundant plasma protein, comprising approximately 60% of total plasma protein mass. It is a single-chain, non-glycosylated polypeptide of 585 amino acids with a molecular weight of 66.5 kDa. HSA is synthesized in the liver at a rate of approximately 13.3 grams per day and has a physiological concentration ranging from 3.0 to 5.0 g/dL (500–750 μM).
The structure of HSA features three homologous domains (I, II, III), each containing two subdomains (A and B). The protein’s flexibility is maintained by 17 conserved disulfide bridges, contributing to an extraordinary ligand-binding capacity. The heart-like crystal structure reveals two primary binding sites: Sudlow’s Site I (warfarin-azapropazone cleft) and Sudlow’s Site II (ibuprofen-diazepam cleft). These hydrophobic cavities contain polar residues at their entrances, enabling interactions with a diverse range of acidic and neutral compounds.
Beyond drug transport, albumin serves multiple physiological functions: maintaining colloidal osmotic pressure, regulating blood pH, providing antioxidant activity through its large thiol pool, and serving as a carrier for endogenous substances including fatty acids, bilirubin, hormones, and metal ions.
Alpha-1-Acid Glycoprotein (AGP)
AGP is the second most important drug-binding protein, with a molecular weight of approximately 42 kDa and consisting of about 45% carbohydrate. Its concentration in plasma is typically 15 μM (0.5–1.0 mg/mL), considerably lower than albumin. Despite its lower concentration, AGP plays a crucial role in binding basic and neutral drugs.
AGP is an acute-phase reactant, meaning its concentration increases significantly in response to inflammation, stress, myocardial infarction, and various disease states. This characteristic has important clinical implications: conditions that elevate AGP can increase drug binding and reduce free drug concentrations.
Lipoproteins & Globulins
High-density lipoproteins (HDL), low-density lipoproteins (LDL), and very-low-density lipoproteins (VLDL) play a more limited role in drug binding compared to albumin and AGP. However, lipophilic drugs, particularly basic compounds, may associate with lipoprotein particles. Alpha, beta, and gamma globulins contribute to drug binding to a lesser extent, though certain hormones and specific drug classes may associate with these proteins.
5. Mechanism of Drug–Protein Binding
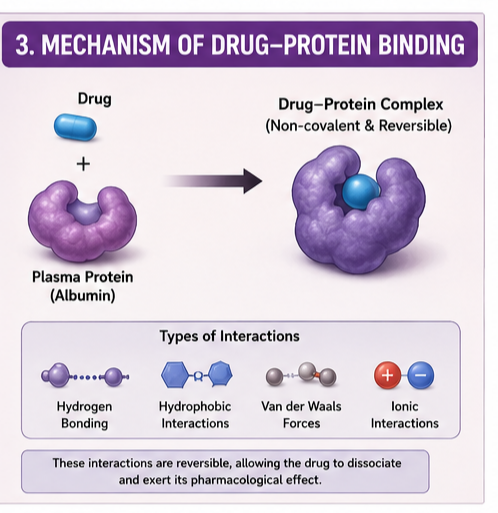 The interaction between drugs and plasma proteins is primarily reversible and occurs through non-covalent forces. These include:
The interaction between drugs and plasma proteins is primarily reversible and occurs through non-covalent forces. These include:
- Hydrophobic interactions – the dominant force for many drug-protein associations, particularly in the hydrophobic pockets of albumin
- Electrostatic interactions – ionic bonds between charged drug molecules and oppositely charged amino acid residues
- Hydrogen bonding – polar residues at binding site entrances form hydrogen bonds with drug molecules
- Van der Waals forces – weak, short-range interactions contributing to binding affinity
Most drugs bind to albumin through Sudlow’s Site I (for bulky heterocyclic anions) or Site II (for aliphatic and aromatic carboxylates). These sites demonstrate stereoselectivity, with enantiomers often displaying different binding affinities. Fatty acids, present at variable concentrations, can competitively displace drugs or induce allosteric conformational changes that alter binding capacity.
6. Bound vs. Free Drug Fraction
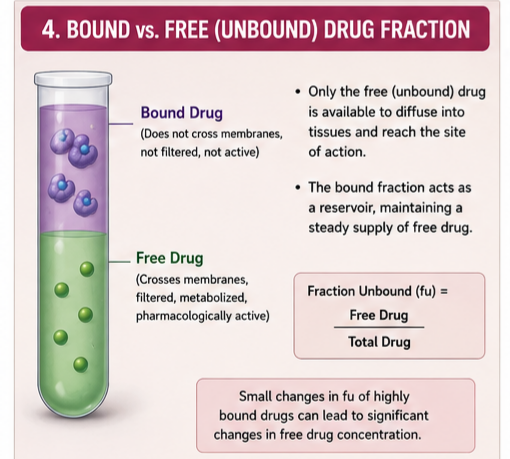 The free drug hypothesis states that only the unbound fraction of a drug is pharmacologically active, capable of crossing cell membranes, metabolized by the liver, and filtered by the kidney. The drug-protein complex cannot permeate through cell membranes by passive transcellular or paracellular permeation.
The free drug hypothesis states that only the unbound fraction of a drug is pharmacologically active, capable of crossing cell membranes, metabolized by the liver, and filtered by the kidney. The drug-protein complex cannot permeate through cell membranes by passive transcellular or paracellular permeation.
The relationship between bound and free fractions is governed by:
Bound Drug = (Protein Concentration × Binding Affinity × Free Drug) / (1 + Binding Affinity × Free Drug)
This equation demonstrates that binding is concentration-dependent and saturable. At therapeutic drug concentrations, most drugs bind without saturating their binding sites; however, for highly bound drugs at high concentrations, saturation can occur, leading to disproportionate increases in free drug concentrations.
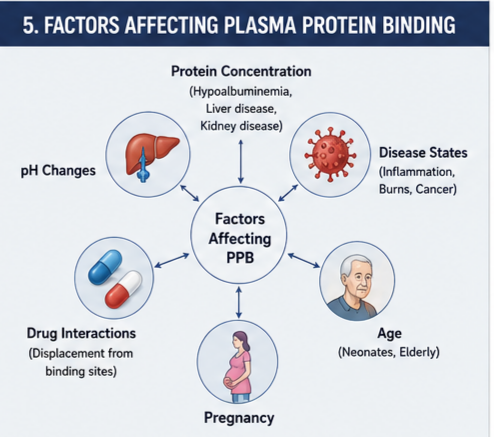
7. Factors Affecting Plasma Protein Binding
Drug-Related Factors
- Lipophilicity – highly lipophilic drugs tend to exhibit greater protein binding
- Acid-base character – acidic drugs preferentially bind to albumin; basic drugs bind primarily to AGP
- Chemical structure – specific molecular recognition elements determine binding affinity
- Concentration – saturable binding can alter the percentage bound at high concentrations
Patient-Related Factors
Liver Disease: Hepatic impairment reduces albumin synthesis, decreasing binding capacity. Additionally, accumulating endogenous substances (bilirubin, bile acids) can compete for binding sites. In alcoholic cirrhosis, both hypoalbuminemia and competitive displacement contribute to increased free fractions of drugs such as phenytoin and diazepam.
Kidney Disease: Uremia alters drug binding through multiple mechanisms: decreased albumin concentration, accumulation of endogenous displacers, and carbamylation of albumin (a post-translational modification that reduces binding affinity). Valproic acid free fraction increases from 8.4% in healthy individuals to 20.3% in renal disease. Similarly, phenytoin free fraction rises from approximately 10% to 24–25% in uraemia.
Pregnancy: Progressive changes occur throughout gestation due to declining albumin concentrations and competitive displacement by endogenous substances. Diazepam free fraction increases from 1.8% in early pregnancy to 2.6% in late pregnancy. Phenytoin free fraction rises from 9.7% to 12.6% as pregnancy advances.
Aging: Age-related physiological changes, including decreased renal function and altered protein concentrations, affect drug binding. While total protein concentrations may change modestly, the quality of binding proteins may be affected. The free fraction of phenytoin increases from 10% to 13.5% with age-related renal function decline.
Critical Illness and Burns: Acute-phase responses elevate AGP concentration, increasing binding of basic drugs. However, critically ill patients often have hypoalbuminemia and accumulate endogenous displacers, creating complex and unpredictable changes in drug binding. A study on critically ill COPD patients showed theophylline free fraction increased from 54.6% to 69.7%.
Hypoalbuminemia and Hyperalbuminemia: Conditions altering albumin concentration directly impact binding capacity. In nephrotic syndrome, diazepam free fraction increases from 1.6% to 3.55%; phenytoin binding is similarly affected. Conversely, factors that increase albumin concentration (rare) would be expected to increase binding.
Pediatric Considerations: Neonates and infants present unique challenges due to immature liver function, lower albumin concentrations, and competition from elevated bilirubin levels. Bilirubin has an association constant 100–1000 times higher than most drugs, displacing bound drugs and increasing free fractions. The unbound cefazolin fraction is significantly higher in neonates than in adults, primarily due to hypoalbuminemia, total plasma concentration, indirect bilirubinemia, and postmenstrual age.
Drug-Drug Interactions: Co-administration of multiple medications can lead to competitive displacement. Drugs with high affinity for binding sites (warfarin, phenytoin, valproic acid) can displace co-administered drugs or be displaced themselves, potentially precipitating toxicity or loss of efficacy.
8. Highly Protein-Bound Drugs (Comparison Table)
A comprehensive analysis of 222 drugs revealed that 50% exhibit 90–100% protein binding. Representative examples include:
| Drug | % Protein Bound | Primary Binding Protein | Clinical Implications |
|---|---|---|---|
| Warfarin | 99% | Albumin | Displacement interactions significant; monitor INR |
| Ibuprofen | 99% | Albumin | Displacement of other drugs possible at high doses |
| Sertraline | 99% | Albumin, AGP | Free concentration monitoring may be useful |
| Tamoxifen | 99% | Albumin, AGP | Extensive binding affects distribution |
| Ketoconazole | 99% | Albumin, AGP | High lipophilicity contributes to binding |
| Salicylic acid | 95% | Albumin | Concentration-dependent binding saturation |
| Clozapine | 95% | Albumin, AGP | Free concentration monitoring recommended |
| Omeprazole | 95% | Albumin | Binding affected by hepatic impairment |
| Fluoxetine | 94% | Albumin, AGP | Extensive binding prolongs half-life |
| Haloperidol | 92% | AGP | Elevated AGP in acute illness reduces free fraction |
| Quinidine | 87% | AGP | Binding increases with AGP concentration |
9. Low Protein-Bound Drugs
Drugs with negligible or minimal binding include acetaminophen (0% bound), fluorouracil (11%), methotrexate (46%), and morphine (35%). These drugs are generally less affected by changes in plasma protein binding, and therapeutic drug monitoring of total concentrations correlates more reliably with clinical effect.
10. Clinical Significance
Effect on Pharmacokinetics
Absorption: Protein binding in the plasma does not directly affect absorption from the gastrointestinal tract but influences the distribution of drug throughout the body after absorption.
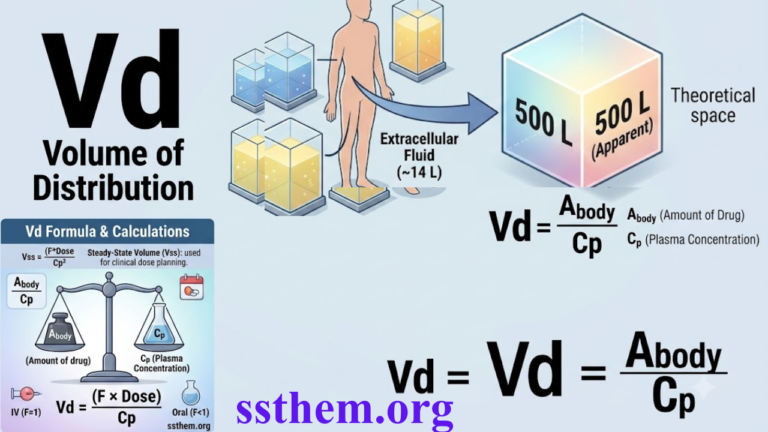
Distribution: Highly protein-bound drugs are largely restricted to the vascular compartment, resulting in low volumes of distribution (Vd). Warfarin, with 99% binding, has a Vd of only 0.1 L/kg. In contrast, drugs sequestered in tissues may have Vd values much higher than total body water, such as propranolol (3.5 L/kg) and digoxin (6 L/kg), despite significant protein binding.
Metabolism: The “restrictive” vs. “permissive” concept describes how protein binding affects hepatic clearance. For drugs with high hepatic extraction (e.g., propranolol, >90% extraction), binding can be “permissive”: extensive binding does not significantly limit clearance because dissociation is rapid. For drugs with low hepatic extraction (e.g., warfarin, <0.3% extraction), binding is “restrictive”: only unbound drug is available for metabolism.
Excretion: Only unbound drug is filtered by the glomerulus and available for active tubular secretion. Highly bound drugs typically have longer elimination half-lives due to reduced clearance. For example, warfarin’s 99% binding contributes to its long half-life.
Effect on Pharmacodynamics
Based on the free drug hypothesis, free drug concentrations correlate best with drug response. This relationship underlies the importance of therapeutic drug monitoring of free (rather than total) concentrations for highly bound drugs.
A sudden increase in free concentration can precipitate toxicity, as occurred with phenytoin when displaced from albumin-binding sites in uraemia. The free fraction increased from approximately 10% to 24–25%, potentially leading to toxicity even with unchanged total concentrations. Dose adjustments in such situations require monitoring of free, not total, drug concentrations.
11. Drug Interactions & Disease Impact
Drug-Drug Interactions
Drug-drug interactions mediated by protein binding can occur through displacement. However, the clinical significance depends on the therapeutic index of the displaced drug, its volume of distribution, and its elimination characteristics. Classical examples include:
- Warfarin displacement: Aspirin and other NSAIDs can displace warfarin from albumin, increasing free warfarin concentration and the risk of bleeding. However, the effect may be transient due to compensatory increased clearance of free drug.
- Phenytoin displacement: Valproic acid displaces phenytoin from albumin, increasing free phenytoin concentration and potentially causing toxicity if total concentration monitoring is used.
- Bilirubin displacement: In neonates, bilirubin can displace drugs from albumin, contributing to higher free fractions and the risk of kernicterus with certain drugs.
Impact of Liver Disease
Hepatic impairment reduces albumin synthesis and alters the competitive environment, typically increasing free drug fractions. In alcoholic cirrhosis, both hypoalbuminemia and competitive displacement contribute to increased free fractions of drugs such as phenytoin and diazepam.
Impact of Kidney Disease
Uremia leads to hypoalbuminemia, accumulation of endogenous displacers, and albumin carbamylation, all reducing binding. The free fraction of phenytoin increases from approximately 10% to 24–25% in uraemia.
Impact of Pregnancy
Progressive changes occur throughout gestation due to declining albumin concentrations and competitive displacement by endogenous substances. Diazepam free fraction increases from 1.8% in early pregnancy to 2.6% in late pregnancy.
Impact of Aging
Age-related physiological changes and decreased renal function can reduce binding for some drugs. The free fraction of phenytoin increases from 10% to 13.5% with age-related renal function decline.
Pediatric Considerations
Neonates have lower albumin concentrations and competitive binding from bilirubin, leading to higher free fractions of many drugs. The unbound cefazolin fraction is significantly higher in neonates than in adults.
Critical Illness & Burns
Acute-phase responses elevate AGP concentration, increasing binding of basic drugs. However, critically ill patients often have hypoalbuminemia and accumulate endogenous displacers, creating complex and unpredictable changes in drug binding.
12. Measurement Methods
Equilibrium Dialysis: Considered the gold standard, equilibrium dialysis uses a semi-permeable membrane to separate bound and unbound drug fractions. The Rapid Equilibrium Dialysis (RED) device has become widely adopted, with equilibration times of 4–6 hours compared to 16–24 hours for conventional methods.
Ultrafiltration: This method uses centrifugal force to separate free drug through a semi-permeable membrane. It is faster than equilibrium dialysis but has limitations: non-specific binding, drug adsorption to membranes, and potential pH shifts during centrifugation.
Ultracentrifugation: This technique uses high-speed centrifugation to sediment plasma proteins, separating them from free drug in the supernatant. It requires specialized equipment and is less commonly used.
Challenges for Highly Bound Compounds: Measuring binding for drugs with >99% binding presents analytical challenges. Novel methods using lipophilic extraction from post-dialysis buffer have been developed for drugs like venetoclax, amiodarone, and montelukast, enabling accurate measurement of extremely low free fractions (fu from 10⁻¹ to 10⁻⁶).
13. Clinical Case Examples
Case 1: Phenytoin in Renal Disease
A patient with chronic kidney disease receiving phenytoin for seizure control: the phenytoin free fraction increases from 10% to approximately 24% in chronic uraemia. Total phenytoin concentration monitoring would underestimate free drug exposure. The clinician should monitor free phenytoin levels to guide dosing and prevent toxicity. Importantly, the increased free concentration is accompanied by increased clearance, potentially maintaining steady-state free concentrations despite altered binding.
Case 2: Valproic Acid in Pregnancy
A pregnant patient on valproic acid for epilepsy: free fraction increases from 9.4% to 14.6% in late pregnancy due to decreased albumin. Total valproic acid levels decrease, potentially leading to dose increases that may not be necessary or may be excessive. Free concentration monitoring is essential.
Case 3: Diazepam in Liver Disease
A patient with alcoholic cirrhosis receiving diazepam: free fraction increases from approximately 2% to 4.5% in uraemia. Clinicians should consider reduced doses for acute use (e.g., status epilepticus), although the large volume of distribution means that for chronic use, monitoring clinical effect is appropriate.
Case 4: Antibiotics in Neonates
A neonate receiving cefazolin: unbound fraction is significantly higher than in adults due to hypoalbuminemia and bilirubin displacement. The dose may need adjustment to achieve similar therapeutic effects, although distribution and clearance changes also require consideration. The association constant of bilirubin for albumin is 100–1000 times higher than for most drugs, making bilirubin displacement clinically significant.
14. Therapeutic Drug Monitoring
For most drugs, monitoring total drug concentrations is sufficient. However, for certain clinical situations, free concentration monitoring is recommended:
- Narrow Therapeutic Index Drugs: Phenytoin, valproic acid, warfarin
- Conditions Altering Protein Binding: Renal disease, hepatic disease, pregnancy, hypoalbuminemia
- Drugs with High Protein Binding: Free monitoring can prevent toxicity or identify subtherapeutic dosing
- Drug-Drug Interactions: When displacement interactions are suspected
The total concentration may not consistently reflect unbound drug concentration in these situations, making free concentration measurement the preferred approach.
15. Common Misconceptions
- Myth 1: Changes in protein binding are always clinically significant.
Reality: For drugs with <80% binding, changes in binding rarely have clinical importance. For highly bound drugs with a wide therapeutic index, binding changes may be clinically insignificant despite being statistically significant. - Myth 2: Total drug concentration is equivalent to active drug concentration.
Reality: Only unbound drug is pharmacologically active and able to cross biological membranes, although total concentrations are often used as a surrogate marker. - Myth 3: Disease-induced changes in binding always require dose adjustment.
Reality: Altered binding may be accompanied by compensatory changes in clearance, maintaining therapeutic effect. The free concentration, not just the extent of binding, determines clinical response. - Myth 4: Highly bound drugs are always long-acting.
Reality: While high binding often prolongs half-life, this is not universal. Drugs with high hepatic extraction (e.g., propranolol) can have short half-lives despite extensive binding. - Myth 5: Displacement interactions always cause toxicity.
Reality: For highly bound drugs with a high hepatic extraction ratio, rapid dissociation allows the displaced drug to be quickly cleared by the liver, preventing significant clinical consequences.
17. Key Takeaways
- Only unbound drug is pharmacologically active and available for metabolism, excretion, and target interaction.
- Albumin and alpha-1-acid glycoprotein are the primary drug-binding proteins, with albumin primarily binding acidic drugs and AGP binding basic and neutral drugs.
- Clinical significance of PPB changes must be evaluated on a drug-by-drug basis; a generalized approach is inappropriate.
- Disease states profoundly affect drug binding: liver disease, renal impairment, pregnancy, aging, and critical illness all alter protein concentrations and binding affinity.
- Highly bound drugs (>90%) are most susceptible to clinically significant binding changes.
- Therapeutic drug monitoring of free, not total, concentrations is recommended for certain drugs in specific patient populations.
- Measurement methods include equilibrium dialysis (gold standard), ultrafiltration, and ultracentrifugation, with RED devices offering improved efficiency.
- Drug-drug displacement interactions can cause toxicity, but the clinical significance depends on the therapeutic index, volume of distribution, and clearance characteristics of the displaced drug.
- Neonates and pregnant patients represent special populations with significantly altered drug binding requiring careful dose adjustment and monitoring.
- Recent research suggests that predictions of free fraction changes based solely on protein concentration changes are insufficient; additional factors, including competitive binding and post-translational modifications, must be considered.
18. References
Major Pharmacology Textbooks
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics. 13th Edition. New York: McGraw-Hill; 2018.
- Katzung BG, Vanderah TW. Basic and Clinical Pharmacology. 15th Edition. New York: McGraw-Hill; 2020.
- Rang HP, Dale MM, Ritter JM, Flower RJ, Henderson G. Rang & Dale’s Pharmacology. 9th Edition. Elsevier; 2019.
- Ritschel WA, Kearns GL. Handbook of Basic Pharmacokinetics. 6th Edition. Washington, D.C.: American Pharmacists Association; 2004.
Clinical Pharmacology Resources
- ASHP (American Society of Health-System Pharmacists). AHFS Clinical Drug Information. Bethesda, MD: ASHP; 2024.
- BNF (British National Formulary). London: BMJ Group and Pharmaceutical Press; 2024.
Regulatory and Health Authority References
- World Health Organization (WHO). WHO Model List of Essential Medicines. Geneva: World Health Organization; 2023.
- US Food and Drug Administration (FDA). Guidance for Industry: Clinical Pharmacology. Silver Spring, MD: FDA; 2023.
- European Medicines Agency (EMA). Guideline on the Pharmacokinetic and Clinical Evaluation of Modified Release Dosage Forms. London: EMA; 2014.
- National Institutes of Health (NIH). Clinical Pharmacokinetics. PubMed; 1976.
Scientific and Clinical Literature
- Bohnert, T., & Gan, L.S. (2010). Significance of Protein Binding in Pharmacokinetics and Pharmacodynamics. Journal of Pharmaceutical Sciences, 99(3), 1107-1122.
- Belinskaia, D.A., et al. (2019). An overview of albumin and alpha-1-acid glycoprotein main characteristics. Heliyon, 5(11), e02879.
- Gogola, D., et al. (2025). Implementation of a novel method for the determination of plasma protein binding of highly bound compounds. Journal of Pharmaceutical and Biomedical Analysis, 256, 116678.
- Zhang, F., et al. (2011). Compilation of 222 drugs’ plasma protein binding data and guidance for study designs. Drug Discovery Today, 16(3-4), 117-123.
- Bteich, M., & Derendorf, H. (2021). Impact of Changes in Free Concentrations and Drug-Protein Binding on Drug Dosing Regimens. Journal of Pharmaceutical Sciences, 110(6), 2372-2383.
- Waters, N.J., et al. (2008). Validation of a rapid equilibrium dialysis approach for the measurement of plasma protein binding. Journal of Pharmaceutical Sciences, 97(10), 4586-4595.
Disclaimer (ڈس کلیمر): یہ تعلیمی مواد صرف معلوماتی مقاصد کے لیے تیار کیا گیا ہے تاکہ فارماکولوجی میں Plasma Protein Binding کے بارے میں سمجھ بوجھ بڑھائی جا سکے۔ یہ کسی بھی قسم کی طبی مشاورت، تشخیص یا علاج کا متبادل نہیں ہے۔ کسی بھی دوائی کا استعمال کرنے سے پہلے ہمیشہ کسی مستند معالج یا فارماسسٹ سے مشورہ کریں۔ اس مضمون میں دی گئی معلومات تازہ ترین سائنسی تحقیقات اور مستند طبی حوالوں پر مبنی ہے تاہم ادویات کے استعمال سے متعلق کوئی بھی فیصلہ کرنے سے پہلے اپنے معالج سے ضرور مشورہ کریں۔
آخری اپ ڈیٹ: جولائی 2026 | ورژن: 2.0 | نظرثانی کی مدت: سالانہ نظرثانی تجویز کردہ
This educational content is for informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always consult your physician or pharmacist before taking any medication.
© 2026 · Plasma Protein Binding in Clinical Pharmacology · All rights reserved.