Volume of Distribution (Vd) Formula, Clinical Importance & Examples in 2026
Volume of Distribution (Vd): Complete Evidence-Based Guide
Volume of Distribution (Vd) is a fundamental pharmacokinetic parameter that quantifies the relationship between the total amount of drug in the body and the drug’s concentration in plasma. It is an apparent volume that reflects the extent to which a drug leaves the vascular compartment and distributes into tissues. Understanding Vd is essential for calculating loading doses, interpreting plasma drug concentrations, and individualising pharmacotherapy in various disease states.
This comprehensive, evidence‑based guide provides a deep dive into Vd — covering its definition, mathematical formulation, physiological determinants, clinical applications, and the impact of patient-specific factors. The content is supported by references from major pharmacology textbooks and peer‑reviewed literature, and is designed for medical students, pharmacists, nurses, and clinicians.
Important: All information is presented for educational purposes only. Always consult a qualified healthcare professional for individualised treatment decisions.
Table of Contents
- 1. Definition of Volume of Distribution
- 2. Why Is Vd Called “Apparent”?
- 3. Historical Background
- 4. Volume of Distribution Formula
- 5. Interpretation of Vd
- 6. Physiological Basis of Drug Distribution
- 7. Factors Affecting Volume of Distribution
- 8. Vd of Common Drugs (Comparison Table)
- 9. Clinical Importance of Vd
- 10. Vd vs Clearance, Bioavailability & Half‑Life
- 11. Clinical Case Examples
- 12. Common Misconceptions
- 13. 50 Frequently Asked Questions (FAQs)
- 14. Key Takeaways
- 15. References
1. Definition of Volume of Distribution
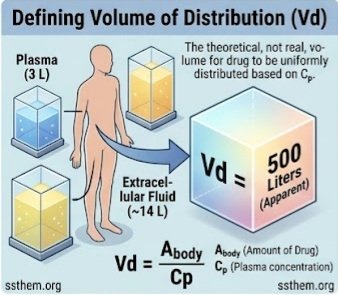 Volume of distribution is formally defined as the apparent volume into which a drug would need to be uniformly distributed to produce the plasma concentration observed. It is a proportionality constant that relates the total amount of drug in the body to the plasma concentration:
Volume of distribution is formally defined as the apparent volume into which a drug would need to be uniformly distributed to produce the plasma concentration observed. It is a proportionality constant that relates the total amount of drug in the body to the plasma concentration:
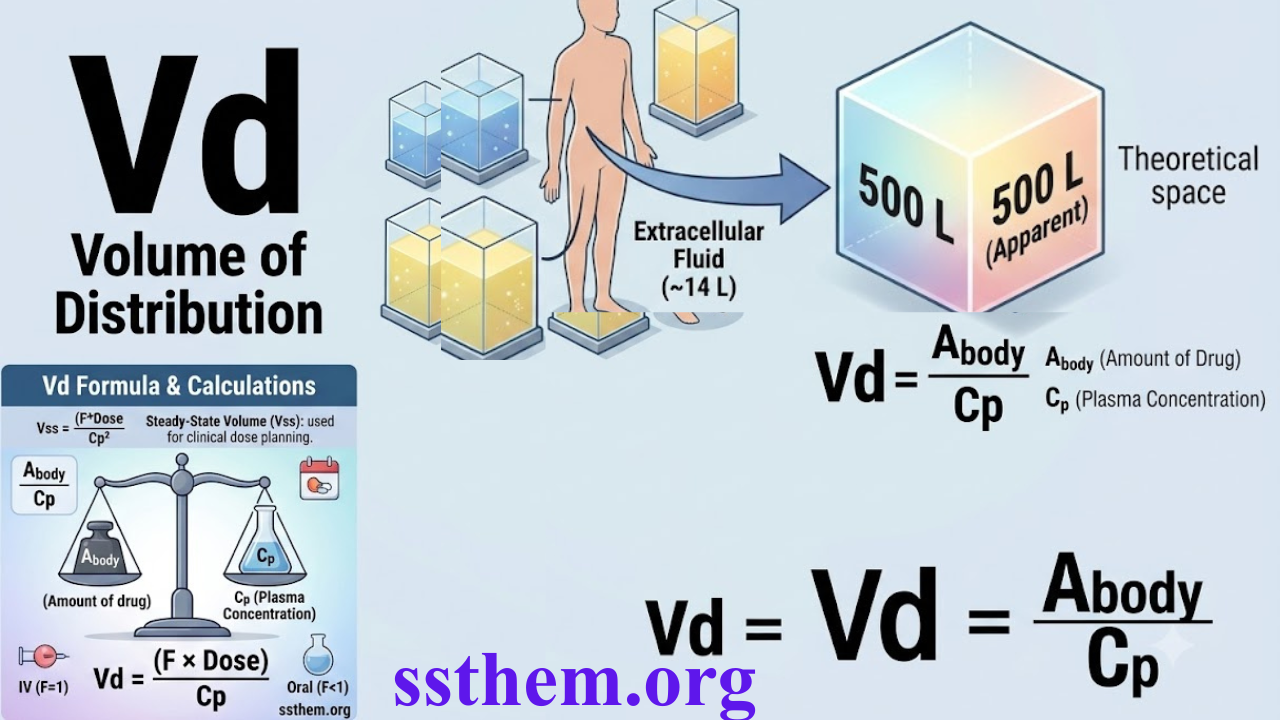
Vd = Amount of drug in the body / Plasma concentration of drug
Vd is expressed in litres (L) or litres per kilogram (L/kg) when normalised to body weight. It is not a real physiological volume but a theoretical construct that reflects a drug’s propensity to leave the vascular compartment and distribute into tissues. For a 70 kg individual, total body water is approximately 42 L, extracellular fluid is ~14 L, and plasma volume is ~3 L. A drug with a Vd of 500 L (e.g., digoxin) clearly cannot be contained in any real anatomical space; the value reflects extensive tissue binding.
Key point: Vd is a proportionality constant, not a measurable physical volume. It provides insight into the distribution characteristics of a drug.
2. Why Is Vd Called “Apparent”?
The term “apparent” underscores that Vd does not correspond to any known anatomical space. The apparent nature arises from several phenomena:
- Tissue binding: Drugs that bind extensively to tissues (e.g., digoxin to skeletal muscle Na⁺/K⁺‑ATPase) are effectively removed from the plasma, lowering measurable plasma concentrations and increasing the calculated Vd.
- Plasma protein binding: Drugs that bind tightly to plasma proteins (e.g., warfarin to albumin) remain in the vascular compartment, increasing measurable plasma concentrations and decreasing Vd.
- Lipophilicity: Highly lipophilic drugs partition into adipose tissue, producing Vd values that greatly exceed total body water (e.g., chloroquine with a Vd of ~235 L/kg).
- Ion trapping: Basic drugs may accumulate in acidic compartments (e.g., lysosomes), further increasing apparent Vd.
For example, chloroquine has a Vd of ~235 L/kg (≈16,450 L for a 70‑kg person) — vastly larger than total body volume — while warfarin has a Vd of only 0.11 L/kg (~8 L), reflecting its high plasma protein binding.
3. Historical Background
The concept of Vd emerged in the mid‑20th century as pharmacokinetic modelling evolved. Early researchers recognised that a simple relationship between dose and concentration could not adequately describe drug behaviour without accounting for distribution. Pioneering work by Torsten Teorell, Eino Nelson, and others established Vd as a distinct parameter, separate from clearance and half‑life. Initially, some authors conflated Vd with clearance, but subsequent research demonstrated that Vd is mechanistically independent of clearance. The development of compartmental modelling introduced multiple Vd terms — Vc (initial or central volume), Vss (steady‑state volume), and Varea (terminal elimination phase volume) — which are now standard in clinical pharmacology.
4. Volume of Distribution Formula
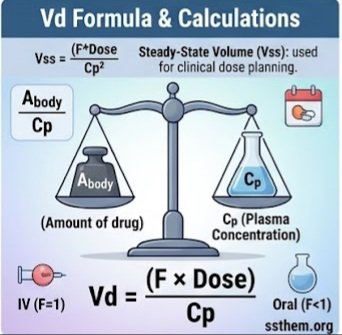
Vd = Abody / Cₚ
Where Abody = total amount of drug in the body (mg), and Cₚ = plasma drug concentration (mg/L). For intravenous administration, Abody equals the administered dose. For extravascular routes, bioavailability (F) must be included:
Vd = (F × Dose) / Cₚ
- Units: litres (L) or litres per kilogram (L/kg) when normalised to body weight.
- Clinical calculation: Vd is determined from concentration‑time data after drug administration, typically using non‑compartmental or compartmental methods.
- Steady‑state Vd (Vss): The most clinically relevant value, calculated as Vss = (Dose × AUMC) / (AUC)², where AUMC is the area under the first moment curve.
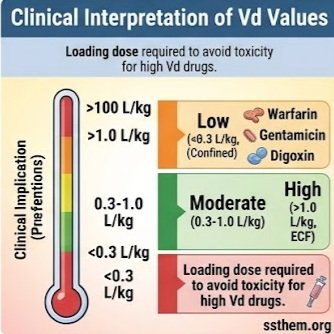
5. Interpretation of Vd
| Vd Range (L/kg) | Interpretation | Examples | Clinical Implication |
|---|---|---|---|
| < 0.3 | Low – drug confined to plasma or extracellular fluid | Warfarin (0.11), Gentamicin (0.25), Tolbutamide (0.11) | Plasma protein binding dominant; dialysis may be effective |
| 0.3 – 0.7 | Moderate – distributes to extracellular fluid | Aminoglycosides, Cisplatin | Fluid shifts can affect dosing |
| 0.7 – 1.0 | Moderate – distributes to total body water | Theophylline (0.5), Ethanol (~0.6), Lithium (~0.8) | Dosing based on total body weight |
| > 1.0 | High – extensive tissue distribution | Digoxin (7), Imipramine (30), Chloroquine (235), Propofol (>100) | Loading dose important; dialysis ineffective |
6. Physiological Basis of Drug Distribution
Drug distribution is the reversible transfer of drug between the intravascular and extravascular compartments. After intravenous administration, a drug first distributes to the central compartment (plasma and highly perfused organs — brain, heart, lung, kidney, liver). From there, it moves to peripheral compartments (muscle, fat, bone, other tissues) at rates governed by blood flow, membrane permeability, and binding affinity.
The relationship between Vd and physiological spaces can be conceptualised:
Vd = Vp + VT × (fu,plasma / fu,tissue)
where Vp = plasma volume, VT = tissue volume, fu,plasma = unbound fraction in plasma, and fu,tissue = unbound fraction in tissue. This equation reveals that Vd increases with tissue binding (low fu,tissue) and decreases with plasma binding (low fu,plasma).
For a drug that does not bind to plasma proteins and distributes freely into total body water, Vd would approximate 0.7 L/kg. Drugs that are highly protein‑bound have Vd values much lower than this, while drugs that bind extensively to tissues have Vd values much higher.
7. Factors Affecting Volume of Distribution
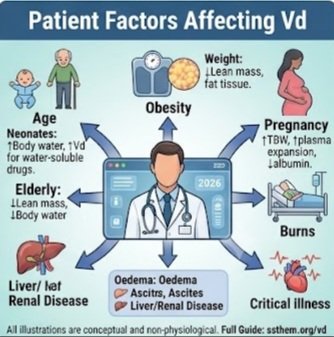
Age
Neonates and infants: Higher total body water (75–80% of body weight vs 50–60% in adults) increases Vd for water‑soluble drugs. Lower plasma protein concentrations and competition from bilirubin also affect binding. The unbound fraction of many drugs (e.g., cefazolin) is significantly higher in neonates.
Elderly: Decreased lean body mass and increased adipose tissue alter Vd. Hydrophilic drugs have reduced Vd, while lipophilic drugs have increased Vd, potentially prolonging half‑life. Age‑related decline in renal function also affects Vd through altered protein binding.
Obesity
Adipose tissue accumulation significantly increases Vd for lipophilic drugs (e.g., propofol, diazepam, amiodarone). Dosing strategies may require different weight scalars:
- Total body weight (TBW): Used for highly lipophilic drugs
- Ideal body weight (IBW): Used for hydrophilic drugs (e.g., gentamicin)
- Adjusted body weight: Used for drugs with moderate lipophilicity
The impact of obesity on Vd is not uniform; drugs with low lipophilicity (e.g., digoxin) show minimal change in Vd with obesity.
Pregnancy
Pregnancy induces profound physiological changes that alter drug distribution:
- Total body water increases by 6–8 litres, peaking at term
- Blood volume increases 30–45%, with maximal expansion at 28–34 weeks
- Plasma albumin concentrations decrease by approximately 10–15%
- Alpha‑1‑acid glycoprotein (AGP) levels may change variably
These changes increase Vd for many drugs, lowering peak concentrations. For example, diazepam free fraction increases from 1.8% in early pregnancy to 2.6% in late pregnancy; phenytoin free fraction rises from 9.7% to 12.6%.
Plasma Protein Binding
Plasma protein binding is a major determinant of Vd. The relationship is mathematically defined in the Vd equation: low fu,plasma (high binding) decreases the tissue:plasma concentration ratio, reducing Vd. Approximately 50% of clinically used drugs are >90% protein‑bound. The primary binding proteins are:
- Albumin: Binds acidic and neutral drugs (e.g., warfarin, diazepam, phenytoin). Concentration ~3.5–5.0 g/dL.
- Alpha‑1‑acid glycoprotein (AGP): Binds basic drugs (e.g., propranolol, lidocaine, imipramine). Concentration ~0.5–1.0 mg/mL; increases as an acute‑phase reactant.
- Lipoproteins: Bind lipophilic drugs (e.g., cyclosporine, certain anaesthetics).
Changes in protein concentration or binding affinity — due to disease, competition, or genetic variation — can significantly alter Vd for highly bound drugs.
Lipophilicity & Water Solubility
Lipophilic drugs (high octanol‑water partition coefficient) readily cross lipid membranes, partition into adipose tissue, and interact with phospholipid membranes, resulting in high Vd. Examples include propofol (>100 L/kg), chloroquine (235 L/kg), and amiodarone (~66 L/kg).
Hydrophilic drugs have limited membrane permeability and remain in the extracellular fluid compartment, resulting in low Vd. Examples include gentamicin (0.25 L/kg), tobramycin, and atenolol (0.7 L/kg).
Ionisation: Drugs that are ionised at physiological pH have reduced membrane permeability. Basic drugs tend to have higher Vd due to interactions with negatively charged phospholipids.
Disease States
Renal Disease: Uraemia alters Vd through multiple mechanisms: fluid retention, decreased plasma protein binding (due to albumin carbamylation and accumulation of endogenous displacers), and altered tissue binding. For phenytoin, free fraction increases from ~10% to 24–25% in uraemia. Valproic acid free fraction increases from 8.4% to 20.3% in renal disease.
Liver Disease: Hepatic impairment reduces albumin synthesis, decreasing binding capacity and increasing free fractions. Ascites and fluid retention expand the extracellular volume, increasing Vd for hydrophilic drugs. In alcoholic cirrhosis, both hypoalbuminaemia and competitive displacement contribute to increased free fractions of drugs such as phenytoin and diazepam.
Burns and Critical Illness: Burn injury increases capillary permeability, allowing drugs and larger molecules to leak into interstitial spaces, increasing Vd. Critically ill patients often have hypoalbuminaemia, elevated AGP (acute‑phase response), and fluid shifts, creating complex and unpredictable changes in Vd.
Heart Failure: Reduced cardiac output decreases tissue perfusion, potentially slowing distribution kinetics and altering apparent Vd. Fluid retention expands the central compartment, affecting Vd for some drugs. Digoxin Vd decreases in heart failure due to reduced muscle mass and perfusion.
Oedema and Ascites: Expanded extracellular fluid volume increases the distribution space for drugs confined to this compartment, affecting Vd calculations.
8. Volume of Distribution of Common Drugs
| Drug | Vd (L/kg) | Vd (70 kg, L) | Key Determinant | Clinical Note |
|---|---|---|---|---|
| Warfarin | 0.11 | 8 | 99% plasma protein binding (albumin) | Low Vd; dialysis ineffective; monitor INR |
| Tolbutamide | 0.11 | 8 | High albumin binding (95%) | Sulphonylurea; binding affected by renal disease |
| Gentamicin | 0.25 | 18 | Hydrophilic, extracellular fluid | Vd increases in fluid overload; monitor trough levels |
| Theophylline | 0.5 | 35 | Total body water distribution | Vd affected by age, heart failure, hepatic disease |
| Atenolol | 0.7 | 49 | Moderate lipophilicity | Hydrophilic beta‑blocker; renally eliminated |
| Lidocaine | 1.7 | 119 | Tissue binding, lipophilicity | High first‑pass metabolism; Vd increased in heart failure |
| Digoxin | 7–8 | 490–560 | Skeletal muscle Na⁺/K⁺‑ATPase binding | Vd reduced in elderly, renal disease; dose by lean weight |
| Imipramine | 30 | 2100 | Lipophilic, extensive tissue binding | Tricyclic antidepressant; high Vd prolongs half‑life |
| Chloroquine | 235 | 16,450 | Lipophilic, fat and tissue sequestration | Exceptionally high Vd; extremely long half‑life |
| Propofol | >100 | >7000 | High lipophilicity, fat distribution | Rapid redistribution; short duration of action |
| Amiodarone | ~66 | ~4620 | Lipophilic, extensive tissue binding | Very long half‑life; large loading dose required |
9. Clinical Importance of Volume of Distribution
Loading Dose Calculation
The most clinically important application of Vd is calculating loading doses to rapidly achieve therapeutic concentrations:
Loading dose = (Cp × Vd) / F
where Cp = desired plasma concentration, and F = bioavailability (F = 1 for IV). Vss (steady‑state Vd) is the most relevant value. Failure to account for Vd can result in subtherapeutic or toxic concentrations.
Therapeutic Drug Monitoring (TDM)
Vd interpretation enables clinicians to understand measured concentrations. A high Vd explains low measured concentrations despite adequate dosing, while a low Vd may indicate concentration‑related toxicity risks. For drugs with high Vd, total concentration monitoring may be misleading; free (unbound) concentration monitoring is preferred for drugs like phenytoin and valproic acid.
Drug Toxicity and Overdose Management
Understanding Vd is critical for managing toxicity:
- Drugs with low Vd (e.g., lithium, gentamicin) are more accessible to dialysis and hemoperfusion.
- Drugs with high Vd (e.g., digoxin, amiodarone, chloroquine) are sequestered in tissues; dialysis is ineffective, and supportive care or specific antidotes are required.
Dose Adjustment in Disease States
Altered Vd in disease states requires dose modification:
- Renal disease: Increased Vd for many drugs may require higher loading doses (e.g., gentamicin in fluid overload).
- Liver disease: Increased Vd for highly protein‑bound drugs may require dose reduction to avoid toxicity.
- Heart failure: Reduced Vd for digoxin requires lower doses.
- Obesity: Weight‑scalar adjustments are essential for appropriate loading doses.
Critical Care Medicine
In critically ill patients, altered physiology (fluid resuscitation, capillary leak, organ dysfunction, altered protein binding) significantly affects drug distribution. Understanding these changes is essential for appropriate dosing in intensive care settings. Many antibiotics require higher loading doses in septic patients due to increased Vd.
10. Vd vs Clearance, Bioavailability & Half‑Life
Vd vs Clearance
Vd and clearance are mechanistically distinct and independent parameters:
- Vd describes the extent of drug distribution.
- Clearance (CL) describes the efficiency of drug elimination (volume of plasma completely cleared per unit time).
They are independent: a drug can have high Vd and low clearance (e.g., amiodarone) or low Vd and high clearance (e.g., metoprolol). This independence has important clinical implications:
- Obesity may increase Vd without altering clearance, prolonging half‑life.
- Liver disease may reduce clearance without affecting Vd.
- Renal failure may decrease both parameters.
Vd vs Bioavailability
Bioavailability (F) is the fraction of an administered dose that reaches systemic circulation unchanged. Vd and F are related through the dosing equation:
Dose = (Cp × Vd) / F
For oral drugs, F affects the effective dose and the calculation of Vd from concentration data.
Vd vs Half‑Life
Half‑life (t₁/₂) is mathematically related to Vd and clearance:
t₁/₂ = (0.693 × Vd) / CL
At constant clearance, a drug with higher Vd has a longer elimination half‑life. This occurs because a greater proportion of the drug resides in peripheral tissues and must redistribute to the central compartment before elimination can occur.
Clinical pearl: Both Vd and clearance are independent variables that collectively determine the dependent variable, half‑life.
11. Clinical Case Examples
Case 1: Warfarin (Low Vd, High Protein Binding)
A 72‑year‑old male with alcoholic cirrhosis and low serum albumin (2.5 g/dL) is prescribed warfarin for atrial fibrillation. Warfarin is 99% albumin‑bound with a Vd of ~0.11 L/kg. The reduced albumin increases the unbound warfarin fraction, potentially intensifying anticoagulation despite a normal total warfarin concentration.
Action: Monitor INR closely; consider lower initial doses. Free warfarin concentration measurement (if available) may guide therapy. The patient’s low albumin also affects other highly bound drugs (e.g., phenytoin, diazepam).
Case 2: Digoxin (High Vd, Tissue Binding)
A 78‑year‑old female with heart failure and reduced skeletal muscle mass (due to age and cachexia) requires digoxin. Digoxin has a Vd of 7‑8 L/kg, primarily due to binding to skeletal muscle Na⁺/K⁺‑ATPase. With reduced muscle mass, the Vd is significantly smaller, and standard loading doses may produce toxic concentrations.
Action: Calculate digoxin dose based on lean body weight (or ideal body weight), not total body weight. Monitor digoxin levels and renal function; consider reduced maintenance doses.
Case 3: Gentamicin in Critical Illness (Increased Vd)
A 45‑year‑old male with septic shock has received 6 litres of fluid resuscitation. Gentamicin (Vd ~0.25 L/kg in healthy individuals) now distributes into an expanded extracellular fluid volume, increasing Vd to ~0.4 L/kg. Standard loading doses may result in subtherapeutic peak concentrations.
Action: Use higher loading doses (e.g., 7 mg/kg actual body weight) to achieve therapeutic peaks; maintenance doses depend on renal function. Therapeutic drug monitoring of peak and trough levels is essential.
Case 4: Phenytoin in Uraemia (Altered Protein Binding)
A patient with chronic kidney disease (CKD) is receiving phenytoin for seizures. In uraemia, phenytoin free fraction increases from ~10% to 24‑25% due to decreased albumin binding (carbamylation, displacers). Total phenytoin levels may appear therapeutic while free levels are toxic.
Action: Monitor free (unbound) phenytoin levels to guide dosing. Free phenytoin targets are 1‑2 mg/L (vs total 10‑20 mg/L). The increased free concentration is accompanied by increased clearance, potentially maintaining steady‑state free concentrations despite altered binding.
12. Common Misconceptions
- Myth: Vd is a real anatomical volume. Reality: Vd is apparent; it can exceed total body volume (e.g., chloroquine Vd = 16,450 L).
- Myth: High Vd means uniform tissue distribution. Reality: The drug may be sequestered in a single tissue (e.g., digoxin in muscle, chloroquine in fat).
- Myth: Vd determines drug effect. Reality: Only unbound drug at the target site produces effect; Vd reflects total drug distribution.
- Myth: Vd and clearance are the same. Reality: They are independent parameters; Vd does not predict clearance.
- Myth: Loading dose is always based on Vd. Reality: For drugs with rapid distribution, Vd (or Vss) is appropriate; for drugs with slow distribution, Vc (central volume) may be more appropriate to avoid toxicity.
- Myth: High Vd always prolongs half‑life. Reality: Half‑life depends on both Vd and clearance; high Vd with high clearance can still have a short half‑life.
- Myth: Vd changes with disease always require dose adjustment. Reality: Altered binding may be accompanied by compensatory changes in clearance; free concentration monitoring is more informative.
Key Takeaways
- Vd is an apparent volume that relates total drug amount to plasma concentration; it is not a real anatomical space.
- High Vd → extensive tissue distribution; low Vd → plasma confinement.
- Drug properties (lipophilicity, ionisation, protein binding) and patient factors (age, obesity, pregnancy, disease) determine Vd.
- Vd is essential for loading dose calculation (Loading dose = Cp × Vd / F) and for interpreting therapeutic drug monitoring results.
- Vd is independent of clearance; both determine elimination half‑life (t₁/₂ = 0.693 × Vd / CL).
- Multiple Vd values exist for multi‑compartment drugs: Vc (initial), Vss (steady‑state), Varea (elimination phase). Vss is most clinically relevant.
- Disease‑induced changes in Vd may require dosage adjustments in renal, hepatic, cardiac, and critically ill patients.
- Free (unbound) concentration monitoring is preferred over total concentration monitoring for highly protein‑bound drugs in disease states that alter binding.
- High Vd drugs are not removed by dialysis; low Vd drugs are accessible for removal in overdose.
- Obesity and pregnancy significantly alter Vd and require weight‑based or adjusted dosing strategies.
15. References
- StatPearls Publishing. Clinical Significance of Volume of Distribution in Pharmacotherapy. In: StatPearls [Internet]. Treasure Island (FL); 2026.
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics. 13th Ed. McGraw‑Hill; 2018.
- Katzung BG, Vanderah TW. Basic and Clinical Pharmacology. 15th Ed. McGraw‑Hill; 2020.
- Rang HP, Dale MM, Ritter JM, Flower RJ, Henderson G. Rang & Dale’s Pharmacology. 9th Ed. Elsevier; 2019.
- Bohnert T, Gan LS. Significance of Protein Binding in Pharmacokinetics and Pharmacodynamics. J Pharm Sci. 2010;99(3):1107‑1122.
- Zhang F, et al. Compilation of 222 drugs’ plasma protein binding data and guidance for study designs. Drug Discov Today. 2011;16(3‑4):117‑123.
- Waters NJ, et al. Validation of a rapid equilibrium dialysis approach for the measurement of plasma protein binding. J Pharm Sci. 2008;97(10):4586‑4595.
- Bteich M, Derendorf H. Impact of Changes in Free Concentrations and Drug‑Protein Binding on Drug Dosing Regimens. J Pharm Sci. 2021;110(6):2372‑2383.
- WHO Model List of Essential Medicines – 2023.
- FDA Guidance for Industry: Clinical Pharmacology – 2023.
- EMA Guideline on the Pharmacokinetic and Clinical Evaluation of Modified Release Dosage Forms – 2014.
Medical Disclaimer (طبّی ڈس کلیمر): This content is for educational and informational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before initiating or changing any pharmacotherapy. The authors and publishers assume no liability for any adverse outcomes resulting from the use or misuse of this information.
Last updated: July 2026 | Version: 2.0 | Review: Annual update recommended.
© 2026 · Volume of Distribution in Pharmacology · All rights reserved.