Drug Distribution in Pharmacokinetics: A Complete Guide for Healthcare Professionals
Drug Distribution: A Comprehensive Pharmacokinetic Guide for Healthcare Professionals
Drug distribution is a fundamental pharmacokinetic process that describes the reversible transfer of a drug from the systemic circulation to the body’s tissues and organs. After a drug enters the bloodstream, its journey to target sites of action is influenced by multiple physiological and physicochemical factors that determine therapeutic efficacy and safety.
Understanding drug distribution is essential for healthcare professionals to make informed decisions about dosing regimens, anticipate drug interactions, and manage therapy in special populations. The process of distribution is dynamic and complex, occurring simultaneously with metabolism and excretion, making it a critical consideration in clinical practice.
This comprehensive guide explores the principles, physiology, and clinical applications of drug distribution, providing evidence-based insights from authoritative sources including the World Health Organization, FDA, EMA, NIH, and leading pharmacology textbooks.
Table of Contents
- 1. Definition of Drug Distribution
- 2. Principles of Drug Distribution
- 3. Physiology of Drug Distribution
- 4. Factors Affecting Drug Distribution
- 5. Plasma Protein Binding
- 6. Volume of Distribution (Vd)
- 7. Blood Flow & Tissue Perfusion
- 8. Biological Barriers
- 9. Tissue Reservoirs
- 10. Redistribution
- 11. Clinical Applications
- 12. Disease Effects on Drug Distribution
- 13. Special Populations
- 14. Drug Interactions Affecting Distribution
- 15. Clinical Case Studies
- 16. Evidence from Clinical Studies
- 17. Tables
- 18. Flowcharts
- 19. Multiple Choice Questions (MCQs)
- 20. Frequently Asked Questions (FAQs)
- 21. Key Takeaways
- 22. References
Definition of Drug Distribution
 Drug distribution can be defined as the reversible transfer of a drug between the blood and the various tissues of the body. This process determines the concentration of a drug at its site of action and influences both therapeutic effects and potential toxicity.
Drug distribution can be defined as the reversible transfer of a drug between the blood and the various tissues of the body. This process determines the concentration of a drug at its site of action and influences both therapeutic effects and potential toxicity.
Distribution is rarely uniform throughout the body. It is characterized by:
- Reversible transfer: Drugs continually move between blood and tissues
- Uneven distribution: Drug concentrations vary significantly between different tissues
- Dynamic equilibrium: Distribution equilibrium is reached when entry and exit rates between blood and tissue become equal
The distribution pattern of a drug is determined by its physicochemical properties (such as lipid solubility, molecular size, and degree of ionization) and physiological factors (including blood flow to tissues, tissue permeability, and protein binding capacity).
Principles of Drug Distribution
Fundamental Concepts
The distribution of a drug throughout the body follows several key principles:
1. Perfusion Rate Limitation
The entry rate of a drug into a tissue depends primarily on the rate of blood flow to that tissue, the tissue mass, and the partition characteristics between blood and tissue. Distribution occurs more rapidly in richly vascularized organs such as the brain, heart, kidneys, and liver compared to poorly perfused tissues like muscle and fat.
2. Permeability Limitation
When a drug cannot easily cross tissue membranes, distribution becomes limited by membrane permeability. This is particularly relevant for drugs that are:
- Highly protein-bound
- Ionized at physiological pH
- Large molecular weight
- Polar (water-soluble) compounds
3. Binding Limitations
The extent of drug distribution into tissues depends significantly on the degree of plasma protein binding and tissue binding. Only the unbound or “free” fraction of a drug is available for distribution to extravascular sites and pharmacologic action.
4. Time-Dependent Distribution
Distribution is not instantaneous; it occurs concurrently with metabolism and excretion. This creates a complex, time-dependent process where drug concentrations in different compartments change continuously following administration.
Physiology of Drug Distribution
Body Water Compartments
For a drug to reach its site of action, it must pass through various fluid compartments in the body. The distribution of a drug can be understood in terms of its access to these body water compartments:
| Compartment | Percentage of Body Weight | Volume in 70kg Adult | Examples of Drugs Distributed |
|---|---|---|---|
| Plasma (Vascular) | ~6% | ~4 L | Heparin, large macromolecules |
| Extracellular Fluid (ECF) | ~20% | ~14 L | Aminoglycosides, hydrophilic drugs |
| Total Body Water | ~60% | ~42 L | Ethanol, small lipophilic molecules |
Drugs with high molecular weight or extensive plasma protein binding remain largely confined to the vascular compartment. Small hydrophilic molecules can cross capillary walls to reach the interstitial fluid but cannot cross lipid cell membranes. Small lipophilic molecules can access total body water, including intracellular fluid.
The Circulatory System’s Role
The circulatory system serves as the primary pathway for drug delivery. Cardiac output distribution to various organs determines the rate and extent of drug distribution:
- High perfusion organs (brain, heart, kidney, liver) receive drugs rapidly
- Moderate perfusion organs (skeletal muscle, skin) receive drugs at intermediate rates
- Low perfusion tissues (fat, bone, cartilage) receive drugs slowly
In clinical settings, conditions such as traumatic injury or inflammation can significantly alter local blood flow, potentially impairing drug delivery to target tissues.
Factors Affecting Drug Distribution
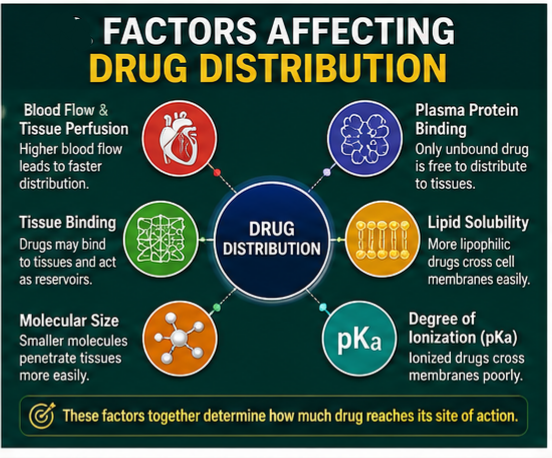
Physiological Factors
1. Blood Flow and Tissue Perfusion
Blood flow is the primary determinant of drug delivery to tissues. Organs with high cardiac output receive drugs more rapidly. This explains why drugs often distribute quickly to the brain, heart, and kidneys before reaching muscle and adipose tissue.
2. Drug Solubility and Physicochemical Properties
A drug’s physical properties significantly influence its distribution pattern:
- Lipid-soluble drugs cross biological membranes readily and distribute more extensively
- Water-soluble drugs have limited membrane penetration and remain more confined to aqueous compartments
- Molecular size affects the ability to pass through capillary endothelial junctions
3. Tissue Binding and Storage
Some tissues can accumulate and store drugs in higher concentrations than others. Tissue reservoirs include:
- Adipose tissue: Stores lipid-soluble drugs (e.g., diazepam, lipid-soluble vitamins)
- Bone and teeth: Bind drugs like tetracycline to calcium salts
- Liver and kidney: Concentrate certain drugs through active transport mechanisms
4. Regional pH Gradients
Variations in tissue pH can affect drug distribution, particularly for weak acids and bases. The degree of ionization at a given pH influences membrane permeability and tissue accumulation.
Physicochemical Factors
1. pKa and Degree of Ionization
Most drugs exist as weak acids or weak bases. Their ionization state at physiological pH affects:
- Membrane permeability (ionized forms are less able to cross lipid membranes)
- Distribution into various body compartments
- Binding to plasma proteins and tissue components
2. Lipophilicity
Lipid-water partition coefficient determines how readily a drug can cross biological membranes. Highly lipophilic drugs:
- Cross the blood-brain barrier easily
- Accumulate in adipose tissue
- Have large volumes of distribution
- May have prolonged effects due to tissue storage
3. Molecular Size
The molecular weight of a drug influences its ability to cross biological membranes. Very large molecules may be restricted to the vascular compartment, while small molecules distribute more freely.
Plasma Protein Binding
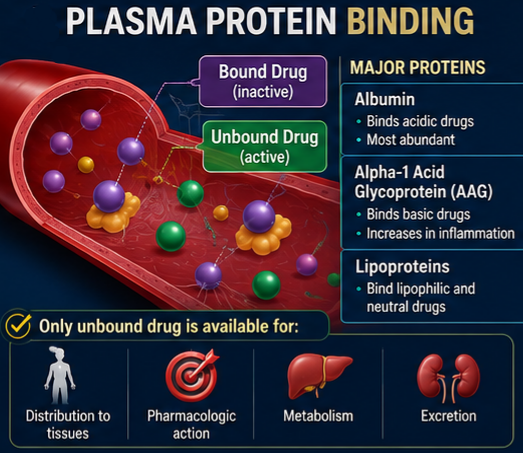
Significance of Protein Binding
In the bloodstream, drugs are transported in two forms:
- Bound drug – reversibly bound to plasma proteins
- Free (unbound) drug – dissolved in plasma water
Only the unbound drug is pharmacologically active and able to:
- Diffuse to extravascular sites
- Cross biological membranes
- Interact with target receptors
- Be metabolized or excreted
Major Drug-Binding Proteins
1. Albumin
- Most abundant plasma protein
- Preferentially binds acidic drugs
- Provides multiple binding sites
- Functions as a drug reservoir
2. Alpha-1 Acid Glycoprotein (AAG)
- Preferentially binds basic drugs
- Levels increase in inflammatory conditions (acute phase reactant)
- Lower concentrations than albumin
3. Lipoproteins
- Bind basic and neutral drugs
- Contribute to distribution of lipophilic compounds
Clinical Implications of Protein Binding
Saturation and Displacement
At high drug concentrations, protein binding sites can become saturated. This forms the basis for:
- Drug-drug interactions: One drug can displace another from binding sites
- Altered free drug concentrations: Saturation leads to increased unbound drug and enhanced effects
Disease Effects
Conditions affecting plasma protein levels alter drug distribution:
- Hypoalbuminemia (e.g., liver disease, nephrotic syndrome): Increases free fraction of acidic drugs
- Acute phase reactions (e.g., malignancy, myocardial infarction): Increase AAG levels, increasing binding of basic drugs
Developmental Factors
Plasma protein binding is reduced in neonates and infants due to:
- Lower albumin and AAG concentrations
- Competition from endogenous substances (bilirubin, free fatty acids)
- Immature binding capacity
Volume of Distribution (Vd)
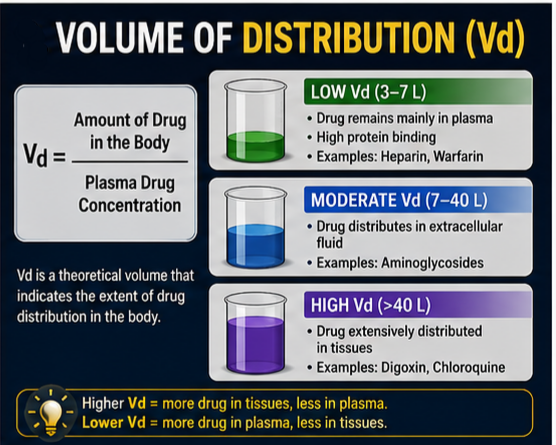
Definition and Calculation
The volume of distribution (Vd) is a theoretical parameter that relates the total amount of drug in the body to the plasma concentration at a given time. It represents the apparent volume into which a drug appears to have distributed.
The formula for Vd is:
Vd = Total amount of drug in the body / Plasma drug concentration
Or for a dose administered:
Vd = D / Cp
where D = dose administered and Cp = plasma concentration.
Clinical Interpretation
The Vd does not correspond to any anatomical space but rather reflects the relative drug affinity for tissues versus plasma compartments.
| Vd Value | Interpretation | Examples |
|---|---|---|
| Low (3-7 L) | Drug remains mainly in plasma | Heparin, warfarin |
| Moderate (7-40 L) | Drug distributes in extracellular fluid | Aminoglycosides |
| High (>40 L) | Drug extensively distributed in tissues | Digoxin, chloroquine |
- Low Vd (< 7 L) indicates extensive plasma protein binding, preventing tissue distribution
- High Vd (may exceed total body water) indicates extensive tissue binding, with little drug remaining in plasma
Factors Affecting Vd
1. Plasma Protein Binding
Drugs with high plasma protein binding tend to have lower Vd. Acidic drugs (e.g., warfarin, aspirin) are highly protein-bound and have small Vd values.
2. Tissue Binding
Drugs with high tissue affinity (e.g., chloroquine in liver cells) have large Vd values. Basic drugs like amphetamine and meperidine are extensively taken up by tissues, giving Vd larger than total body volume.
3. Lipophilicity
Highly lipophilic drugs partition into adipose tissue, increasing Vd.
4. Disease States
Critical illness may alter Vd through:
- Increased total body water
- Decreased plasma protein concentrations
- Tissue perfusion changes
- Extravascular fluid collections (e.g., ascites, pleural effusions)
Blood Flow & Tissue Perfusion
Distribution Based on Perfusion Rate
The rate at which a drug enters a tissue is primarily determined by blood flow, unless diffusion across cell membranes is rate-limiting. Tissue perfusion varies widely throughout the body:
High Perfusion Tissues (Rapid Distribution)
- Brain (receives ~15% of cardiac output)
- Heart
- Kidneys
- Liver
- Lungs
Intermediate Perfusion Tissues
- Skeletal muscle
- Skin
Low Perfusion Tissues (Slow Distribution)
- Adipose tissue
- Bone
- Cartilage
Clinical Significance
Relevance in Drug Action
The rapid onset of effect for many drugs (particularly those acting on the central nervous system) is due to high perfusion of target organs. For example, the rapid anesthetic effect of thiopental results from its swift distribution to the highly perfused brain.
Drug Accumulation
Poorly perfused tissues can serve as depots, slowly accumulating drugs over time. This has clinical implications:
- Prolonged drug action may result from slow release from tissue stores
- Repeated dosing may lead to significant accumulation in fat tissue
Biological Barriers
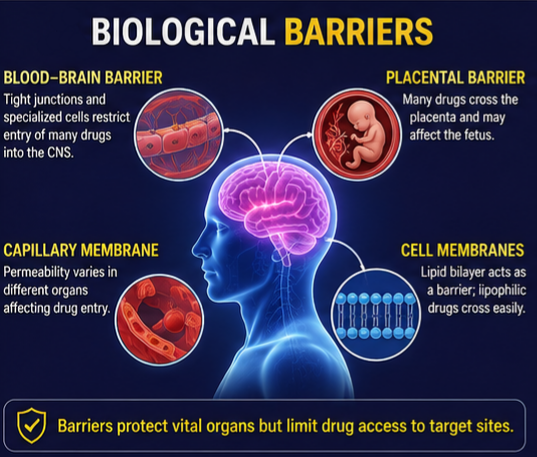
The Blood-Brain Barrier (BBB)
The blood-brain barrier is a specialized structure that restricts drug entry into the central nervous system (CNS). It consists of:
- Tight junctions between capillary endothelial cells
- Astrocytic sheath surrounding the capillary endothelium
- Limited fenestration of brain capillaries
Factors Affecting BBB Penetration:
- Lipid solubility: Lipid-soluble drugs (e.g., thiopental) enter the brain readily
- Molecular size: Small molecules penetrate more easily
- Protein binding: Highly protein-bound drugs have limited entry
- Ionization: Polar compounds and ionized drugs cross poorly
Age-Related Changes
The blood-brain barrier may become less effective with aging, allowing increased passage of compounds into the brain. This can affect drug sensitivity in elderly patients.
The Placental Barrier
The placental barrier regulates drug transfer between maternal and fetal circulation. Characteristics include:
- Permeability: Many drugs cross the placenta, especially lipid-soluble compounds
- Transporters: Some drugs are actively transported across the placenta
- Clinical implications: Pregnant women require careful consideration of drug distribution to the fetus
Membrane Permeability
Biological membranes act as barriers to drug distribution. The rate of passage depends on:
- Lipid solubility: The primary determinant of passive diffusion
- Molecular size: Smaller molecules diffuse more readily
- Charge: Ionized drugs cross membranes poorly
- Carrier-mediated transport: Some drugs use transporters to cross membranes
Tissue Reservoirs
Definition and Clinical Significance
Tissue reservoirs are sites where drugs accumulate in concentrations higher than in plasma. These reservoirs serve as storage depots, releasing the drug slowly back into circulation as plasma concentrations decline.
Major Tissue Reservoirs
1. Adipose Tissue
- Stores lipid-soluble drugs
- Examples: Diazepam, barbiturates, lipid-soluble vitamins
- Due to poor perfusion, equilibration is slow
2. Bone and Teeth
- Bind tetracyclines to calcium salts
- Can cause discoloration of developing teeth in children
- Prolonged retention due to low turnover
3. Liver and Kidney
- Actively concentrate certain drugs
- Example: Chloroquine concentrations in liver cells can be thousands of times higher than in plasma
Clinical Implications

Prolonged Drug Action
Accumulation in tissue reservoirs can extend drug effects. For example:
- Thiopental initially produces rapid anesthesia but terminates as the drug redistributes to fat storage
- Alendronate remains in bone for 4-7 months after administration stops
Repeated Dosing Concerns
If doses are repeated, drug accumulation in tissues can reach clinically significant levels, potentially leading to:
- Extended pharmacologic effects
- Enhanced toxicity
- Prolonged drug interactions
Redistribution
Mechanism of Redistribution
Redistribution is the process by which drugs initially distributed to highly perfused organs subsequently move to less perfused tissues. This phenomenon explains the termination of action for many drugs with rapid onset.
Example: Thiopental
- Initial distribution: Highly lipid-soluble, rapidly enters the brain after IV injection
- Rapid effect: Marked anesthetic effect within seconds
- Redistribution: Effect ends within minutes as thiopental redistributes to fat tissue
- Slow release: Gradually released from fat, maintaining subanesthetic levels
Clinical Significance
Drugs with Redistribution Properties
- Thiopental and other barbiturates
- Propofol
- Fentanyl and other highly lipophilic opioids
Implications for Dosing
- Initial dose requirements may be higher to achieve therapeutic effect
- Repeated dosing can lead to tissue accumulation
- Elimination may be prolonged after extended use due to depot release
Clinical Applications
Dosing Implications
Understanding drug distribution is critical for rational drug dosing:
1. Loading Doses
The volume of distribution determines the loading dose required to achieve a desired plasma concentration:
- Loading dose = Vd × target concentration
- Drugs with large Vd require larger loading doses
2. Maintenance Dosing
Distribution affects:
- Dosing frequency
- Time to steady state
- Fluctuation in drug levels
3. Therapeutic Drug Monitoring
Interpretation of plasma concentrations must consider:
- Individual Vd variations
- Effects of disease on distribution
- Special population considerations
Drug Interactions Affecting Distribution
Mechanisms of Distribution Interactions
1. Protein Binding Displacement
- Occurs when two drugs compete for protein binding sites
- Clinically significant when drug is >90% protein-bound and Vd is small (<0.15 L/kg)
- Transient increase in free drug concentration may enhance effects
- Net result at steady state: unchanged free concentration, decreased total concentration
Examples of Clinically Significant Displacement
- Warfarin displaced by other highly protein-bound drugs
- Phenytoin displaced by valproic acid
- Bilirubin displacement by sulfonamides (risk of kernicterus in neonates)
Monitoring of Free Drug Concentrations
For drugs that are highly protein-bound and subject to therapeutic monitoring (e.g., phenytoin), measuring free drug concentrations is more clinically relevant than total concentrations when:
- Protein binding is altered (e.g., in hypoalbuminemia, renal failure)
- Drug interactions affect binding
- Drug monitoring results are difficult to interpret
Disease Effects on Drug Distribution
Renal Disease
Effects on Distribution
- Decreased albumin levels (nephrotic syndrome)
- Increased Vd for acidic drugs
- Accumulation of endogenous substances competing for binding sites
- Uremic toxins may affect protein binding
Clinical Implications
- Increased free fraction of acidic drugs
- Potential toxicity at normal total concentrations
- Need for therapeutic drug monitoring of free concentrations
- Dosage adjustment based on renal function
Liver Disease
Effects on Distribution
- Impaired albumin synthesis → hypoalbuminemia
- Increased Vd for acidic drugs
- Altered protein binding
- Changes in regional blood flow
- Ascites may create additional drug reservoir
Clinical Implications
- Enhanced pharmacologic response due to increased free drug
- Potential for toxicity
- Need for dosage adjustment
- Monitoring of free concentrations recommended
Inflammatory States and Acute Phase Response
Effects on Distribution
- Elevated alpha-1 acid glycoprotein levels
- Increased binding of basic drugs
- Decreased Vd for basic drugs
- Altered response to basic drugs
Clinical Implications
- Reduced pharmacologic effect of basic drugs
- Higher doses may be required
- Conditions include: malignancy, myocardial infarction, inflammatory bowel disease, infections
Critical Illness
Effects on Distribution
- Increased total body water (edema, fluid resuscitation)
- Altered plasma protein levels
- Variable tissue perfusion
- Extravascular fluid collections (ascites, pleural effusions)
- Altered capillary permeability
Clinical Implications
- Unpredictable drug distribution
- Need for careful therapeutic drug monitoring
- Individualized dosing based on response and monitoring
Special Populations
Pediatric Patients
Unique Distribution Characteristics
1. Body Composition
- Higher percentage of extracellular fluid volume (up to 440 mL/kg in neonates vs. 200 mL/kg in adults)
- Lower percentage of body fat (increases with age)
- Relatively larger organs (liver, brain)
2. Protein Binding
- Lower plasma protein concentrations, especially in neonates
- Decreased albumin binding capacity until approximately 12 months of age
- Competition from endogenous substances (bilirubin, free fatty acids)
3. Clinical Implications
- Higher weight-normalized doses often required for hydrophilic drugs
- Increased Vd for many drugs in neonates
- Monitoring of free drug concentrations when clinically relevant
Elderly Patients
Distribution Changes in Aging
1. Body Composition
- Decreased total body water
- Decreased lean body mass
- Increased percentage of body fat
- Effects on drug distribution vary by lipophilicity
2. Protein Binding
- Decreased serum albumin
- Increased alpha-1 acid glycoprotein (in inflammatory states)
- Altered drug binding capacity
3. Clinical Implications
- Increased Vd for lipophilic drugs (e.g., diazepam, some benzodiazepines)
- Decreased Vd for hydrophilic drugs (e.g., digoxin, alcohol)
- Enhanced sensitivity to protein-bound drugs
- Prolonged drug effects due to accumulation in fat
Pregnancy
Distribution Changes
1. Physiological Changes
- Increased total body water
- Increased cardiac output
- Decreased albumin concentrations
- Altered regional blood flow
2. Fetal Considerations
- Placental transfer of drugs
- Variable fetal distribution
- Accumulation in fetal tissues
3. Clinical Implications
- Changes in Vd during pregnancy
- Altered dosing requirements
- Potential fetal exposure
- Consideration of pregnancy category and fetal risks
Obesity
Distribution Changes
1. Body Composition
- Increased adipose tissue
- Increased total body water in adipose tissue (though proportionally lower)
- Variable lean body mass
2. Clinical Implications
- Increased Vd for lipophilic drugs
- Dosing based on actual body weight may lead to toxicity
- Dosing based on ideal or adjusted body weight recommended for many drugs
- Studies necessary for determining optimal dosing in obese patients
Drug Interactions Affecting Distribution
Protein Binding Interactions
Mechanisms
Competition for limited binding sites on plasma proteins leads to displacement of one drug by another. This increases the free fraction of the displaced drug.
Conditions for Clinical Significance
- Drug is >90% protein-bound
- Drug has clearance that is capacity-limited and binding-sensitive
- Vd is small (typically <0.15 L/kg)
Examples of Clinically Significant Interactions
| Displaced Drug | Displacer Drug | Potential Effect |
|---|---|---|
| Warfarin | Aspirin | Increased anticoagulant effect, bleeding risk |
| Phenytoin | Valproic acid | Increased free phenytoin, toxicity |
| Sulfonamides | Bilirubin | Risk of kernicterus in neonates |
Tissue Binding Interactions
Some drugs may compete for tissue binding sites, potentially affecting distribution and toxicity. However, these interactions are generally less well-characterized than protein binding interactions.
Transporter Interactions
Drug transporters (e.g., P-glycoprotein, organic anion transporting polypeptides, organic cation transporters) play an increasingly recognized role in drug distribution. Interactions at transport sites can affect tissue distribution and drug response.
Clinical Case Studies
Case Study 1: Phenytoin Therapy in a Patient with Hypoalbuminemia
Patient Profile
- 72-year-old male with cirrhosis and hypoalbuminemia (albumin 2.0 g/dL)
- Epilepsy requiring phenytoin therapy
- Therapeutic drug monitoring shows total phenytoin 6 mcg/mL (therapeutic range 10-20 mcg/mL)
Clinical Question
Why does the patient continue experiencing seizures despite total phenytoin concentration below therapeutic range?
Pharmacokinetic Analysis
- Phenytoin is highly protein-bound (~90%), primarily to albumin
- Hypoalbuminemia reduces total binding capacity
- Despite low total concentration, free (unbound) concentration may be therapeutic
- Standard total drug monitoring underestimates free drug concentration
Management
- Measure free phenytoin concentration (therapeutic range 1-2 mcg/mL)
- If free concentration is appropriate, monitor clinically and maintain current dose
- If seizures persist despite therapeutic free concentration, consider alternative therapy
Case Study 2: Thiopental Redistribution
Patient Profile
- 45-year-old female undergoing anesthesia induction
- Thiopental 4 mg/kg IV administered
- Rapid loss of consciousness within 30 seconds
- Patient awakens after 5-10 minutes
Pharmacokinetic Analysis
- Thiopental is highly lipid-soluble, rapidly crosses the blood-brain barrier
- Initial distribution to brain produces rapid anesthetic effect
- Redistribution to adipose tissue terminates CNS effect
- Low perfusion of fat tissue means slow equilibration
Clinical Implications
- Duration of effect is short (minutes) after a single dose
- Despite awakening, significant drug may remain in adipose tissue
- Repeated doses may cause accumulation and prolonged effects
Case Study 3: Digoxin Therapy in Renal Failure
Patient Profile
- 68-year-old female with chronic kidney disease (GFR 25 mL/min)
- Heart failure requiring digoxin therapy
- Loading dose administered using standard protocol
Clinical Question
Why does the patient develop digoxin toxicity despite appropriate loading dose?
Pharmacokinetic Analysis
- Digoxin has a large Vd (~5-7 L/kg)
- Vd may be decreased in renal failure (less lean body mass, altered tissue binding)
- Reduced renal clearance leads to higher plasma concentrations
- Standard loading dose based on estimated Vd may be excessive
Management
- Adjust loading and maintenance doses based on renal function
- Monitor digoxin concentrations closely
- Consider reduced dose and extended intervals
- Monitor for signs of toxicity
Evidence from Clinical Studies
The Role of Distribution in Drug Development
Clinical studies demonstrate that understanding drug distribution is essential for drug development programs at both preclinical and clinical stages. Key study findings include:
Pharmacokinetic Studies
- Distribution studies using radiolabeled drugs reveal tissue distribution patterns
- Understanding Vd is critical for predicting drug accumulation and half-life
- Tissue distribution data inform safety and efficacy assessments
Therapeutic Drug Monitoring
- Clinical studies have established therapeutic ranges and monitoring requirements
- Individual factors affecting distribution influence interpretation of drug levels
Special Population Studies
- Age, disease, and genetic factors affect drug distribution
- Clinical trials in special populations help establish appropriate dosing guidelines
Guidelines from Regulatory Authorities
US FDA Guidance
- Recommends pharmacokinetic studies in special populations
- Requires characterization of protein binding for new drugs
- Emphasizes the importance of tissue distribution in safety assessment
EMA Recommendations
- Requires distribution studies for drug approval
- Emphasizes characterization of distribution in vulnerable populations
- Provides guidance on pediatric pharmacokinetic studies
Tables
Table 1: Factors Affecting Drug Distribution and Clinical Implications
| Factor | Mechanism | Clinical Implication | Example |
|---|---|---|---|
| Blood Flow | High flow = rapid distribution | Faster drug action | Thiopental → rapid brain distribution |
| Tissue Binding | Accumulation in tissues | Prolonged action | Tetracycline in bone |
| Plasma Protein Binding | Only free drug is active | Interactions possible | Warfarin displacement |
| Lipophilicity | High = wider distribution | Long half-life | Diazepam fat storage |
| Molecular Size | Large = limited distribution | Restricted to vascular | Heparin in plasma |
Table 2: Volume of Distribution Values for Common Drugs
| Drug | Vd (L/kg) | Interpretation | Primary Factors |
|---|---|---|---|
| Heparin | 0.05-0.1 | Very low | High molecular weight, plasma binding |
| Warfarin | 0.1-0.2 | Low | High plasma protein binding |
| Phenytoin | 0.6-0.8 | Moderate | Plasma binding, tissue distribution |
| Digoxin | 5-7 | High | Extensive tissue binding |
| Chloroquine | 100-1000 | Very high | Massive tissue accumulation |
| Diazepam | 1.5-2.5 | Moderate-high | Lipophilicity, fat storage |
Table 3: Disease Effects on Protein Binding
| Disease | Protein Affected | Effect on Binding | Clinical Impact |
|---|---|---|---|
| Cirrhosis | Albumin | ↓ Binding of acidic drugs | ↑ Free concentrations of acidic drugs |
| Nephrotic Syndrome | Albumin | ↓ Binding of acidic drugs | ↑ Free concentrations of acidic drugs |
| Inflammatory Disease | AAG | ↑ Binding of basic drugs | ↓ Free concentrations of basic drugs |
| Malignancy | AAG | ↑ Binding of basic drugs | ↓ Free concentrations of basic drugs |
| Neonatal Status | Albumin, AAG | ↓ Binding capacity | ↑ Free concentrations of many drugs |
| Renal Failure | Albumin | Altered binding | ↓ Binding, ↑ free concentrations |
Table 4: Distribution in Special Populations
| Population | Body Water Changes | Fat Changes | Protein Changes | Vd Impact |
|---|---|---|---|---|
| Neonates | ↑ ECF volume | ↓ Body fat | ↓ Binding capacity | ↑ Vd for hydrophilic drugs |
| Elderly | ↓ TBW | ↑ Body fat | ↓ Albumin | ↑ Vd for lipophilic drugs |
| Pregnancy | ↑ TBW | ↑ Body fat | ↓ Albumin | ↑ Vd for some drugs |
| Obesity | ↑ TBW | ↑ Adipose | Variable | ↑ Vd for lipophilic drugs |
Flowcharts
Flowchart 1: Drug Distribution and Pharmacokinetics
[DRUG ADMINISTRATION]
↓
[SYSTEMIC CIRCULATION]
↓
┌────────────┐
│ FACTORS AFFECTING DISTRIBUTION │
│ • Blood flow to tissues │
│ • Capillary permeability │
│ • Plasma protein binding │
│ • Tissue binding │
│ • Lipid solubility │
│ • Molecular size │
│ • Drug transporters │───────────┘
↓
[DISTRIBUTION TO TISSUES]
↓
───────────┐
│ DISTRIBUTION PATTERNS │
│ • High perfusion organs (rapid) │
│ • Low perfusion tissues (slow) │
│ • Barrier-limited distribution (BBB) │
│ • Tissue accumulation (reservoirs) │
↓
[DRUG AT SITE OF ACTION]
↓
[PHARMACOLOGIC EFFECT]
Flowchart 2: Factors Determining Volume of Distribution
[DRUG ADMINISTRATION]
↓
[DOSE (mg)] / [PLASMA CONCENTRATION (mg/L)]
↓
───────────┐
│ VOLUME OF DISTRIBUTION (Vd) │
│ Apparent Volume (L or L/kg) │
└────────────┐
│ DETERMINANTS OF Vd │ │
│ HIGH Vd (Large) LOW Vd (Small) │
│ • Extensive tissue • High plasma │
│ binding protein binding │
│ • High lipophilicity • Low lipophilicity │
│ • Low plasma • Large molecular │
│ protein binding weight │
│ • Small molecular • High polarity │
│ weight │
│ CLINICAL SIGNIFICANCE
├──────────────────
│ • Loading dose = Vd × target concentration │
│ • Half-life affected by Vd │
│ • Steady-state fluctuation dependent on Vd │
│ • Disease effects require dose adjustment │
└──────────────────
Flowchart 3: Drug Distribution Barriers
[DRUG IN CIRCULATION]
↓
│ BIOLOGICAL BARRIERS │ │
│ 1. CAPILLARY ENDOTHELIUM │
│ • Continuous capillaries │
│ • Fenestrated capillaries │
│ • Sinusoidal capillaries │
│ 2. BLOOD-BRAIN BARRIER │
│ • Tight junctions │
│ • Astrocytic sheath │
│ • Transporters │
│ 3. PLACENTAL BARRIER │
│ • Lipid barrier │
│ • Transport systems │
│ 4. CELL MEMBRANES │
│ • Phospholipid bilayer │
│ • Protein channels │
│ • Transporters
↓
[TISSUE PENETRATION]
↓
┌──────────────────
│ FACTORS AFFECTING │
│ BARRIER PENETRATION
├──────────────────
│ • Lipid solubility │
│ • Molecular size │
│ • Degree of ionization │
│ • Protein binding │
│ • Carrier-mediated transport │
│ • Membrane permeability
Question 1: Which of the following best describes the volume of distribution (Vd)?
A) The actual volume of body water in which a drug is dissolved
B) A theoretical volume relating the amount of drug in the body to plasma concentration
C) The volume of blood in which a drug is distributed
D) The volume of adipose tissue that binds a drug
Answer: B Explanation: Volume of distribution is an apparent, theoretical volume that relates the total amount of drug in the body to its plasma concentration. It is not an actual anatomical volume but rather a reflection of the relative distribution of a drug between plasma and tissues.
Question 2: Which drug property would result in the highest volume of distribution?
A) High plasma protein binding
B) Low lipophilicity
C) High tissue binding
D) High molecular weight
Answer: C Explanation: High tissue binding pulls drug out of the plasma compartment, decreasing plasma concentration and increasing the calculated volume of distribution. Extensive tissue binding is a major determinant of high Vd values.
Question 3: The blood-brain barrier restricts the entry of drugs due to:
A) Fenestrated capillaries
B) Tight junctions between endothelial cells
C) High blood flow to the brain
D) Lipophilic drug properties
Answer: B Explanation: Brain capillary endothelial cells have tight junctions that restrict the passage of water-soluble and protein-bound drugs. Lipid-soluble drugs can cross more readily. Tight junctions are the anatomical basis for the barrier.
Question 4: Which of the following statements about plasma protein binding is true?
A) Only the bound drug is pharmacologically active
B) The bound drug can cross biological membranes
C) Only the unbound drug is pharmacologically active
D) Binding is irreversible
Answer: C Explanation: Only the unbound (free) fraction of a drug is pharmacologically active, able to cross membranes, and available for metabolism and excretion. Protein binding is reversible and occurs in equilibrium.
Question 5: What is the clinical significance of drug redistribution?
A) It always prolongs drug effects
B) It can explain the short duration of action of some drugs
C) It only occurs in the liver
D) It is not clinically relevant
Answer: B Explanation: Redistribution from highly perfused organs to less perfused tissues can terminate the effect of rapidly acting drugs. This explains the short duration of action for drugs like thiopental.
Question 6: In which patient population is the volume of distribution for hydrophilic drugs most likely to be increased?
A) Elderly patients
B) Obese patients
C) Neonates
D) Young adults
Answer: C Explanation: Neonates have a higher percentage of extracellular fluid volume compared to adults (440 mL/kg vs. 200 mL/kg), leading to a larger Vd for hydrophilic drugs that distribute primarily in the extracellular compartment.
Question 7: A drug with high protein binding and low volume of distribution is likely to:
A) Have a long half-life
B) Be susceptible to displacement interactions
C) Distribute extensively to tissues
D) Have low concentration in plasma
Answer: B Explanation: High protein binding with low Vd means the drug is largely confined to the plasma compartment and is susceptible to displacement by other drugs that compete for protein binding sites. This can lead to clinically significant interactions.
Question 8: Which of the following factors would increase drug distribution to the brain?
A) High protein binding
B) High lipid solubility
C) Large molecular size
D) High degree of ionization
Answer: B Explanation: High lipid solubility allows drugs to cross the blood-brain barrier readily. Protein-bound drugs, large molecules, and ionized compounds have limited brain distribution.
Question 9: Tissue reservoirs are clinically significant because:
A) They always increase drug toxicity
B) They can prolong drug action as drug is slowly released
C) They have no effect on drug therapy
D) They increase drug metabolism
Answer: B Explanation: Tissue reservoirs act as depots, releasing drug slowly back into circulation as plasma concentrations decline. This can prolong drug effects and be clinically relevant, especially with repeated dosing or when considering withdrawal effects.
Question 10: In hypoalbuminemic patients, which of the following is expected?
A) Decreased free fraction of acidic drugs
B) Increased free fraction of acidic drugs
C) No change in drug binding
D) Increased binding of basic drugs
Answer: B Explanation: Hypoalbuminemia reduces the binding capacity for acidic drugs, increasing the free (unbound) fraction. This can lead to enhanced pharmacologic effects and potential toxicity.
- Definition and mechanism: Drug distribution is the reversible transfer of drugs between blood and tissues, determining concentrations at sites of action.
- Clinical importance: Understanding distribution is crucial for proper dosing, route selection, drug interaction management, and individualised therapy.
- Volume of distribution: Vd is a theoretical parameter reflecting drug distribution patterns. High Vd indicates extensive tissue distribution; low Vd suggests confinement to plasma.
- Plasma protein binding: Only unbound drug is pharmacologically active. Disease states, drug interactions, and developmental factors can alter protein binding.
- Biological barriers: The blood-brain barrier and placental barrier restrict drug entry to certain tissues, affecting drug selection and dosing.
- Special populations: Neonates, elderly, pregnant women, and obese patients exhibit altered distribution patterns requiring careful dose selection.
- Disease effects: Conditions such as hypoalbuminemia, liver disease, renal disease, and inflammatory states can lead to unexpected drug responses.
- Clinical applications: Distribution principles guide loading dose calculations, drug interaction prediction, and individualised therapy.
- Monitoring: Therapeutic drug monitoring is valuable for drugs subject to altered distribution, particularly those with narrow therapeutic windows.
- Patient variability: Genetic polymorphisms, age, disease, and concomitant medications contribute to interindividual variation in drug response.
References
Major Pharmacology Textbooks
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics. 13th Edition. New York: McGraw-Hill; 2018.
- Katzung BG, Vanderah TW. Basic and Clinical Pharmacology. 15th Edition. New York: McGraw-Hill; 2020.
- Rang HP, Dale MM, Ritter JM, Flower RJ, Henderson G. Rang & Dale’s Pharmacology. 9th Edition. Elsevier; 2019.
- Ritschel WA, Kearns GL. Handbook of Basic Pharmacokinetics. 6th Edition. Washington, D.C.: American Pharmacists Association; 2004.
Clinical Pharmacology Resources
- ASHP (American Society of Health-System Pharmacists). AHFS Clinical Drug Information. Bethesda, MD: ASHP; 2024.
- BNF (British National Formulary). London: BMJ Group and Pharmaceutical Press; 2024.
Regulatory and Health Authority References
- World Health Organization (WHO). WHO Model List of Essential Medicines. Geneva: World Health Organization; 2023.
- US Food and Drug Administration (FDA). Guidance for Industry: Clinical Pharmacology. Silver Spring, MD: FDA; 2023.
- European Medicines Agency (EMA). Guideline on the Pharmacokinetic and Clinical Evaluation of Modified Release Dosage Forms. London: EMA; 2014.
- National Institutes of Health (NIH). Clinical Pharmacokinetics. PubMed; 1976.
Scientific and Clinical Literature
- Balant L, et al. Clinical Pharmacokinetics. Schweiz Med Wochenschr. 1976;106(2):33-42.
- Bjornsson TD. Practical uses of individual pharmacokinetic parameters in drug development and clinical practice: examples and simulations. Eur J Drug Metab Pharmacokinet. 1997 Jan-Mar;22(1):1-12.
- Oie S. Drug distribution and binding. J Clin Pharmacol. 1986 Nov-Dec;26(8):583-7.
- Giacomini KM, Huang SM, Tweedie DJ, et al. Membrane transporters in drug development. Nat Rev Drug Discov. 2010;9:215-236.
- Rodgers T, Rowland M. Mechanistic approaches to volume of distribution predictions: understanding the processes. Pharm Res. 2007;24(5):918-933.
- Grover A, Benet LZ. Effects of drug transporters on volume of distribution. AAPS J. 2009;11(2):250-261.
Disclaimer (ڈس کلیمر): یہ تعلیمی مواد صرف معلوماتی مقاصد کے لیے تیار کیا گیا ہے تاکہ فارماکولوجی میں Drug Distribution کے بارے میں سمجھ بوجھ بڑھائی جا سکے۔ یہ کسی بھی قسم کی طبی مشاورت، تشخیص یا علاج کا متبادل نہیں ہے۔ کسی بھی دوائی کا استعمال کرنے سے پہلے ہمیشہ کسی مستند معالج یا فارماسسٹ سے مشورہ کریں۔ اس مضمون میں دی گئی معلومات تازہ ترین سائنسی تحقیقات اور مستند طبی حوالوں پر مبنی ہے تاہم ادویات کے استعمال سے متعلق کوئی بھی فیصلہ کرنے سے پہلے اپنے معالج سے ضرور مشورہ کریں۔
آخری اپ ڈیٹ: جولائی 2026 | ورژن: 2.0 | نظرثانی کی مدت: سالانہ نظرثانی تجویز کردہ
This educational content is for informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always consult your physician or pharmacist before taking any medication.
© 2026 · Drug Distribution Guide · All rights reserved.